In a shop that specializes in horse supplements in which I buy glycine, they sell a microcapsule form of vitamin C, according to information on the site this form of vitamin C is released only in the intestine, as the shell is ethylcellulose it is not digested in the stomach. The vitamin is osmotically released by diffusion from the capsule. The coating does not affect the absorption. The level of absorption is 99%. Thanks to the encapsulated form, it is possible to administer many times higher doses of vitamin C than in its traditional form, without causing digestive disorders. The price is also not high, around 30 euros per kilo
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
High Dose Intravenous Vitamin C (and other vitamin infusions)
- Thread starter Laura
- Start date
beetlemaniac
The Living Force
I've also known a doctor here in Malaysia who specializes in using IV Vitamin C to treat all types of cancers. He's found really good results with it and the stories he has are remarkable. My uncle, who was from the same class as this doctor during university years, is more of a mainstream practitioner, but he admitted with some fear the power IV Vitamin C against cancers though he still doesn't seem to fully accept it. Maybe his stance has changed since I last spoke to him about this.
This is the page on his website on the intravenous therapy.
This is the page on his website on the intravenous therapy.
Well, it sounds like a vitamin C or sodium ascorbate enema might be very helpful? Another line to investigate, I think.
Rectal enema is specifically recommended for unconscious people in an emergency when is hard to find veins. Children are good candidates in this regard.
I just bought some sodium ascorbate and I will be "investigating it" this weekend. I'll report if I notice any results worth mentioning.
I'd like to collect specific protocols here if some of y'all can find them and copy/paste in this thread. How much for how many days, for how long, for what condition (not just cancer), and what results expected?
I wrote a summary back in 2013 to collect this data:
Vitamin C's Historical and Miraculous Record | The Health Matrix
... I compiled this record of the early pioneers in an effort to learn from their experiences and to get an idea of how much they used, when and how....
-150 grams reversed pathology in a given case and was the amount given over a period of 24 hours. The I.V. was continuous and it was given in three bottles of 5 Dextrose water, removing only the water in c.c. to be replaced by the ‘C’ ampoules.
-It is a powerful oxidizer and when given in massive amounts of 50 grams to 150 grams, intravenously, for certain pathological conditions, and “run in” as fast as 20 Gauge needle will allow, it acts as a “Flash Oxidizer,”often correcting the pathology within minutes. Ascorbic acid is also a powerful reducing agent. Its neutralizing action on certain toxins, exotoxins, virus infections, endotoxins and histamine is in direct proportion to the amount of the lethal factor involved and the amount of ascorbic acid given. At times it is necessary to use ascorbic acid intramuscularly. It should always be used orally, when possible, along with the needle.
-To determine the degree of the body’s saturation of vitamin C, the capillary fragility test which is similar to the tourniquet test can be used as a guide. It can be used to estimate the quantity of vitamin C necessary to maintain capillary integrity.
-In 1953, a case history was presented of a patient with viral pneumonia, unconscious, with a fever of 106.8°F when admitted to the hospital. 140 grams ascorbic acid was given intravenously over a period of 72 hours at which time she was awake, sitting up in bed and taking fluids freely by mouth. The temperature was normal.
-The permeability of the blood-brain barrier can be compromised by toxic agents in the blood circulation. The integrity of the capillary wall in regulating permeability of the blood vessels of the central nervous system is crucial. Ascorbic acid will repair and maintain the integrity of the capillary wall.
-After severe burns there is considerable alteration in the metabolism of ascorbic acid. There is an increase demand for ascorbic acid in burns especially when epithelization and formation of granulation tissue are taking place. Limited amounts of ascorbic acid to a dose range of 300 mg to 2000 mg daily, in divided doses, have been capable of hastening the healing of wounds by producing healthy granulation tissue and also by reducing local edema. It also made antibiotic therapy rarely necessary. A 3% ascorbic acid solution as a spray over the entire area of the burn can be used every 2 to 4 hours for a period of roughly five days. Dr. Klenner suggested IV vitamin C at the dose of 500 mg per Kg. body weight diluted to at least 18 c.c. per gram vitamin C using 5% dextrose in water, saline in water or Ringers solution and for the initial injection, run in as fast as a 20 gauge needle or catheter will carry the flow. Cut-downs are frequently necessary and the foot-ankle area is recommended. Vitamin C solution is repeated every 8 hours for the first several days, then at 12 hour intervals. Ascorbic acid, by mouth, is given to tolerance. Loose stools is accepted as this index. Using large doses of ascorbic acid I.V. will necessitate the administration of at least one gram calcium gluconate, daily, to replace free calcium ions removed in the breakdown chemical action as ascorbic acid goes to dehydroascorbic acid, then to ketogulonic acid and later to oxalic acid as the calcium salt.
–Pseudomonas will not be a problem, since ascorbic acid destroys the exotoxin systemically and locally. Even if the burn is seen late when pseudomonas is a major problem the gram negative bacilli will be destroyed in a few days leaving a clean healthy surface. Dr. Klenner reported having seen eschars 2 inches wide and 1/2 inch thick, severely infected so that stench had to be controlled with deodorizing sprays, melt away when employing the method outlined. Ascorbic acid also eliminates pain so that opiates or their equivalent are not required.
-During pregnancy, requirements were roughly 4 grams first trimester, 6 grams second trimester and 10 grams third trimester. Hemoglobin levels were much easier to maintain. Leg cramps were less frequent. Striae gravidarum was seldom encountered. Labor was shorter and less painful. There were no postpartum hemorrhages. The perineum was found to be remarkably elastic and episiotomy was performed electively. Healing was always by first intention and even after 15 and 20 years following the last child the firmness of the perineum is found to be similar to that of a primigravida in those who have continued their daily supplemental vitamin C.
Regarding they myth that ascorbic acid enhances kidney stone formation…
-Chief factors in the formation of renal calculi are perversions of metabolic processes, infection and stasis in the urinary tract. Stasis and a concentrated urine appear to be the chief physiological factors. The only way that oxalic acid can be produced from ascorbic acid is through splitting of the lactone ring. This happens above pH5. The reaction of urine when 10 grams of vitamin C is taken daily is usually pH6. Oxalic acid precipitates out of solution only from a neutral or alkaline solution-pH7 to pH10. Ingestion of 9 grams ascorbic acid daily resulted in oxalate spills as high as 68 mg for 24 hours and in the controls without extra vitamin C the high was 64 mg for a 24 hour period.
-The amount of oxalic acid found in the diabetic patient approximates that found in the urine of a normal person taking 10 grams vitamin C each day. Give this individual 10 grams ascorbic acid daily, by mouth, and the urinary oxalate excretion remains relatively unchanged. Diabetics are known for their diuresis. The individual who takes 10 or more grams of vitamin C each day will find that this organic compound is an excellent diuretic. No urinary stasis; no urine concentration.
-The clinical value of ascorbic acid in combating shock is explained by the inhibition of deaminizing enzymes from the damaged cells by vitamin C. Conditions of shock and stress cause depletion of the ascorbic acid content of the plasma. As with the virus bodies, ascorbic acid also joins with the protein factor of these toxins effecting quick destruction. Large amounts of ascorbic acid 350 mg to 700 mg per Kg. body weight are given intravenously. In small patients, where veins are at a premium, ascorbic acid can easily be given intramuscularly in amounts up to two grams at one site. Several areas can be used with each dose given. Ice held to the gluteal muscles until red, almost eliminates the pain. The ice is reapplied for a few minutes after the injection. Ascorbic acid is also given, by mouth, as follow-up treatment.
-Every diabetic not taking supplemental vitamin C could be classified as having sub-clinical scurvy. For this reason they find it difficult to heal wounds. The diabetic patient will use the supplemental vitamin C for better utilization of his insulin. It will assist the liver in the metabolism of carbohydrates and to reinstate his body to heal wounds like normal individuals. 60% of all diabetics could be controlled with diet and 10 grams ascorbic acid daily. The other 40% will need much less needle insulin and less oral medication.
-Samples of blood taken six hours after surgery showed vitamin C drops of approximately 1/4 the starting amount and at 12 hours the levels were down to one-half. Optimal primary wound healing is dependent to a large extent upon the vitamin C content of the tissues. In a hopeless surgical situation, two grams of ascorbic acid was given by syringe every two hours for 48 hours and then 4 times each day. In 36 hours the patient was walking the halls and in seven days was discharged with normal elimination and no pain. She has outlived her surgeon by many years. All patients should take 10 grams ascorbic acid each day. Where this is not done and the surgery is elective, then 10 grams by mouth should be given for several weeks prior to surgery. At least 30 grams should be given, daily, in solutions, post-operatively, until oral medication is allowed and tolerated.
-Large doses of intravenous “C” has a striking influence on the course of mononucleosis. In one patient who was given the last rites of her church, the girls mother took things into her own hands when the attending physician refused to give ascorbic acid. In each bottle of intravenous fluids she would quickly “tap in” 20 to 30 grams vitamin C. The patient made an uneventful recovery.
-In the presence of ascorbic acid, carcinogenic metabolites of bladder cancer will not develop in the urine. Ascorbic acid will control myelocytic leukemia provided 25 to 30 grams are taken orally each day. At least one research team has demonstrated that in cancer all available “C” is mobilized at the site of the malignancy. “How long must we wait for someone to start continuous ascorbic acid drip for 2 to 3 months, giving 100 to 300 grams each day, for various malignant conditions?” asks Dr. Klenner.
How long indeed! Almost a century later, we still wonder.
-Vitamin C is a regulator of the rate at which cholesterol is formed in the body; deficiency of the vitamin speeding the formation of this substance. In experimental work, guinea pigs fed a diet free of ascorbic acid showed a 600 percent acceleration in cholesterol formation in the adrenal glands.
-Back then, massive intravenous ascorbic acid therapy were given to patients with infectious hepatitis and patients were well and back to work in from 3 to 7 days. In these cases the vitamin was also employed by mouth as follow-up therapy. 10 grams daily, intravenously, proved the best treatment available.
-One single injection of ascorbic acid calculated at 500 mg per Kg. body weight will reverse heat stroke.
-One to three injections of the vitamin in a dose range of 400 mg Kg. body weight will effect a dramatic cure in Virus Pancarditis.
-One gram taken every one to two hours during exposure will prevent sunburn.
-Intravenous injections will quickly relieve the pain and erythema, even the second degree burns when precautions are not taken.
-One to three injections of 400 mg per Kg. given every eight hours will “dry up” chicken-pox in 24 hours.
-Injections are usually given with a syringe in a dilution of one gram to 5 c.c fluid. This concentration will produce immediate thirst. This is prevented by having the patient drink before giving the injection.
-40 grams ascorbic acid by vein and 1000 mg to 2000 mg vitamin B1 intramuscularly will neutralize the person intoxicated by alcohol.
-5 per cent ointment using a water soluble base will cure acute fever blisters if applied 10 or more times a day and several small basal cell epithelioma cancer has been removed with a 30 percent ointment.
-Very promising results were reported in glaucoma with a dose schedule of 100 mg per Kg. body weight taken after meals and bed hour.
-In arthritis at least 10 grams daily and those taking 15 to 25 grams daily will experience commensurate benefit. Supportive treatment must also be given. Repair of collagenous tissue is dependent of adequate ascorbic acid.
-Complications of smallpox vaccination are usually handled by adequate oral ascorbic acid. Sometimes “C” intravenously was needed.
-In massive “shingles” ascorbic acid should also be given by vein. Always as much by mouth as can be tolerated. Heavy metal intoxication is also resolved with adequate vitamin C therapy.
-General all around benefits of one to ten grams ascorbic acid per day. It has been suggested that ascorbic acid metabolism may be an index of total metabolism and thus serve as a general diagnostic guide. Adults taking at least 10 grams of ascorbic acid daily, and children under ten at least one gram for each year of life will find that the brain will be clearer, the mind more active, the body less wearied and the memory more retentive.
-Ascorbic acid destroys virus bodies by taking up the protein coat so that new units cannot be made, by contributing to the break-down of virus nucleic acid with the result of controlled purine metabolism.
-The clinical use of vitamin C in pneumonia has a very sound foundation. The larger the dose of ascorbic acid the better were the results. A schedule of one gram each hour for 48 hours and then 10 grams each day by mouth. Those under ten at least one gram for each year of life.
-In Virus Encephalitis a dose schedule of from 350 mg to 700 mg per Kg. body weight diluted to at least 18 c.c. of 5D water to each gram of “C” is recommended. In small children, 2 and 3 grams can be given intramuscularly, every 2 hours. An ice cap to the buttock will prevent soreness and induration. Ascorbic acid in amounts under 400 mg per Kg. body weight can be administered intravenously with a syringe in dilutions of 5 c.c. to each one gram provided the ampoule is buffered with sodium bicarbonate with sodium Bisulfite added. As much as 12 grams can be given in this manner with a 50 c.c. syringe. Larger amounts must be diluted with “bottle” dextrose or “saline” solutions and run in by needle drip. This is true because amounts like 20 to 25 grams which can be given with a 100 c.c. syringe can suddenly dehydrate the cerebral cortex so as to produce convulsive movements of the legs. This represents a peculiar syndrome, symptomatic epilepsy, in which the patient is mentally clear and experiences no discomfiture except that the lower extremities are in mild convulsion. This epileptiform type seizure will continue for 20 plus minutes and then abruptly stop. Mild pressure on the knees will stop the seizure so long as pressure is maintained. If still within the time limit of the seizure the spasm will reappear by simply withdrawing the hand pressure. Dr. Klenner saw this in two patients receiving 26 grams intravenously with a 100 c.c. syringe on the second injection. One patient had poliomyelitis, the other malignant measles. Both were adults. He duplicated this on himself to prove no after effects. Intramuscular injections are always 500 mg to 1 c.c. solution. With continuous intravenous injections of large amounts of ascorbic acid, at least one gram of calcium gluconate must be added to the fluids each day. This is done because we have found that massive doses of ascorbic acid pulls free calcium ions from the vicinity of the platelets or from the calcium-prothrombin complex as the lactone ring of dehydroascorbic acid is opened. The first sign of calcium ion loss is “nose bleeding”. This differs from the nosebleed found, at times, in cases of chicken pox or measles. Here it represents frank scurvy from vitamin C deficiency. The pathology being “Capillary fragility”.
-Multiple uses for ascorbic acid include Cardiovascular Diseases, Hypermenorrhea, Peptic and Duodenal Ulcers, Post-operative and Radiation Sickness, Rheumatic Fever, Scarlet Fever, Poliomyelitis, Acute and Chronic Pancreatitis, Tularemia, Whooping Cough and Tuberculosis. In one case of scarlet fever in which Penicillin and the Sulfa drugs were showing no improvement, fifty grams ascorbic acid given intravenously resulted in a dramatic drop in the fever curve to normal. Here the action of ascorbic acid was not only direct but also as a synergist. A similar situation was observed in a case of lobar pneumonia. In another case of puerperal sepsis following a criminal abortion the initial dose of ascorbic acid was 1200 mg per Kg body weight and two subsequent injections were at the 600 mg level. Along with Penicillin and Sulfadiazine an admission temperature of 105.4°F. was normal in nine hours. The patient made an uneventful recovery. In one spectacular case of Black Widow spider bite in a 3 1/2 year old child, in coma, one gram calcium gluconate and 4 grams of ascorbic acid was administered intravenously when first seen in the office. Four grams ascorbic acid was then given every six hours using a 20 c.c. syringe. She was awake and well in 24 hours. Physical examination showed a comatose child with a rigid abdomen. The area about the umbilicus was red and indurated, suggesting a strangulated hernia. With a 4 power lens, fang marks were in evidence. Thirty hours after starting the vitamin C therapy the child expelled a large amount of dark clotted blood. There was no other residual. A review of the literature confirmed that this individual has been the only one to survive with such findings; the others were reported at autopsy. Ten grams vitamin C and 200 mg to 400 mg vitamin B-6, by mouth, daily will “shield” one from mosquito bites.
-Ascorbic acid must be given by needle to bring about quick reversal of various “insults” to the human body. Doses must range from 350 mg to 1200 mg per Kg body weight. Under 400 mg per Kg of body weight the injection can be made with a syringe provided the vitamin is buffered with sodium bicarbonate with Sodium Bisulfite added. Above 400 mg doses per Kg body weight, the vitamin must be diluted to at least 18 c.c. of 5 per cent dextrose in water, saline in water or Ringer’s solution. In debilitated individuals or when the pathology is serious, cortisone therapy was also used.
–Pesticide Poisoning. A 12 year old boy was given 10 grams of ascorbic acid with a 50 c.c. syringe every 8 hours. The concentration was one gram for each 5 c.c. diluent. He was returned home on the second hospital day.
–Nasal Diphtheria. A little girl was given 10 grams ascorbic acid, intravenously, with a 50 c.c. syringe every 8 hours for the first 24 hours and then every 12 hours for two times. She was then put on one gram ascorbic acid every two hours by mouth.
–Poliomyelitis. Two brothers were sick with poliomyelitis. These two boys were given 10 and 12 grams of ascorbic acid, according to weight, intravenously with a 50 c.c. syringe, every eight hours for 4 times and then every 12 hours for 4 times. They also were given one gram every two hours by mouth around the clock. They made complete recovery.
–Virus infection. Adequate ascorbic acid therapy must be continued long enough to destroy all virus bodies, otherwise the infection will recur.
–Snake bite. Child of 4 years was struck on the lower leg by a large highland moccasin at 7:00 P.M., while at play in the yard of her country home. Four grams of ascorbic acid was given intravenously at 7:35 P.M. with a 20 c.c. syringe. The following 25 minutes were taken to follow a skin test on anti-venom. At this time and before the anti-venom was administered the child had stopped vomiting, she had stopped crying and was sitting on the emergency room table, laughing and drinking a glass of orange juice. Seen in the office at 10:00 A.M. the following morning she still demonstrated the small amount of swelling of her leg and had 1/2 degree fever. She was given a second dose of 4 grams of ascorbic acid intravenously. Seen at 5 P.M. she had no fever but the swelling remained constant. There was no pain. The following day, 38 hours after being bitten, she was completely normal. An additional 4 grams of ascorbic acid was given on this visit. No other antibiotics were given and none was required.
–Monoxide Poisoning. 12 grams ascorbic acid with a 50 c.c. syringe using a 20 gauge needle. (We employ a 20 G. needle when using a 50 c.c. syringe; 21 G needle for a 30 c.c. syringe; 22 G needle for a 20 c.c. syringe and a 23 G needle for a 10 c.c. syringe. This assists in controlling the rate of flow which is important, especially, in young children). Within 10 minutes the patient was awake, sitting up on the edge of the examining table, rubbing his eyes and saving: “Doc, what in the world am I doing up here in your office.” He returned to his place of employment within 45 minutes.
–Acute Virus pancarditis. A five year old boy was admitted to the local hospital with history of having a “relapse” after recovery from measles. The physical findings showed a thready and feeble pulse. A distinct rub was in evidence by auscultation. The EKG showed RS-T deviations. The temperature was 105°F.. Ascorbic acid calculated at 400 mg per Kg body weight was given intravenously with a syringe. Within two hours the picture had almost reverted to normal. Injection of Vitamin C was repeated in 6 hours and again at 12 hours. A fourth injection was given after 24 hours although the patient was clinically well. The child returned home on the 4th hospital day.
–Acute pancreatitis. Adult Male seen in the emergency room of local hospital complaining of severe, agonizing pain in the epigastrium which radiated to the back. Nausea and vomiting were present. Serum amylase studies showed a concentration of 345. This was the 4th such attack experienced by this patient. Sixty grams ascorbic acid in 700 c.c. Dextrose in water was given intravenously. 20 mg Pantapon was given in the emergency room. No additional opiates were required. The patient made an uneventful recovery. He was placed on 10 grams ascorbic acid by mouth and has not had a recurrence in almost 5 years. He has, however, developed mild diabetes mellitus which is now controlled with diet and vitamin C.
-“A scientific idea must live dangerously or die of inanition. Science thrives on daring generalizations. There is nothing particularly scientific about excessive caution. Cautious explorers do not cross the Atlantic of truth.”-Lancelot Hogben
Continues below...
Vitamin C's Historical and Miraculous Record | The Health Matrix
[Snipped the part on oral doses. Very important info though!]
Clinical Guide to the Use of Vitamin C by Lendon H. Smith, M.D.
These are the Clinical Experiences of Frederick R. Klenner, M.D., as abbreviated, sumarized and annotated by
Lendon H. Smith, M.D.. You can read the full article here.
-The patient should “get large doses of Vitamin C in all pathological conditions while the physician ponders the diagnosis.”
-If we base our needs on the amounts other mammals manufacture with their intact enzyme it comes to 2-4 grams daily in the unstressed condition. Under stress 70 kg of rats make 15 grams of C.
-If you are hypoascorbemic because you cannot manufacture Vitamin C from sugar, extra glucose in your diet will not help, you need to take Vitamin C.
-Vitamin C level of the blood plasma fell to zero for 90 days before there was obvious clinical evidence and that this was as long as 132 days before the first signs appeared.
-As an oxidizing agent massive amounts, i.e., 5-150 grams, intravenously, for certain pathological conditions.
-Vitamin C acts as a reducing agent, an oxidizing agent, an anti-clotting agent, an antihistamine, and as an anti-infective agent.
-Ascorbic acid enters all cells. It “proceeds to take up the protein coats being manufactured by the virus nucleic acid, thus preventing the assembly of new virus units.”
-Failure to benefit from Vitamin C use is usually due to inadequate amounts being used for too short a period of time.
-Vitamin C combines directly with the toxin/virus. This new compound is oxidized by Vitamin C; the toxin/virus and the Vitamin C are destroyed. This must be why C has to be continued after the apparent cure.
-The anaerobic condition in the tissue is relieved. Acidity is decreased and large amounts of Adrenaline disappear. The constriction of the blood vessels ceases and the liver and pancreas can receive the proper nutrients to function. Properly calculated doses of C on a continuing basis will restore the normal physiology of the body.
-The adrenals and Vitamin C are interrelated.
-Patients ill with a virus would show petechial hemorrhages (small leaks of blood into the skin) when a tourniquet was applied to increase venous backpressure. Capillary weakness is a sign of low levels of Vitamin C.
-The collagen of all fibrous tissue structures is dependent on an adequate level of Vitamin C. These weak capillary walls may allow a simple virus to invade the brain
-Vitamin C acts as catalyst in the assimilation of iron.
A note of caution: Those with iron overload (ask your physician to test for ferritin, transferrin, TIBC and iron) should keep in mind that vitamin C increases the absorption of iron into the body, especially in the heart where it can cause heart failure, palpitations and others. Ferritin levels should be ideally less than 80 and transferrin saturation should be less than 40%. If you are above those levels, you might want to donate some blood or refer to the Iron Disorders Institute. A great book on the subject is The Elephant Iron by Roberta Crawford.
-Ascorbic acid is a necessary coenzyme in the metabolic oxidation of tyrosine. The latter is necessary to break down protein to a usable amino acid.
-Highly alkaline urine has less Vitamin C. The Vitamin C would be thus retained in the tissues helping to guard against the viruses and bacteria. When Vitamin C levels drop, glycogen in the liver is converted to glucose: a response to stress.
-The usual dose of 65 mg per kilogram of body weight may be expected to take care of the usual virus infection when given every 2-4 hours by needle. The more severe condition would respond to larger single injections.
-However “if the activity of the pathogen is completely stopped, the development of active immunity will be interrupted.” Therefore, modification of childhood diseases is the aim of Vitamin C treatment, not the complete overnight suppression that would prevent the body from making immune memory. To accomplish modification, 250 mg per kilogram should be given intramuscularly. If necessary, half of this amount would be given in eight hours. Procaine 1.5-2% can be given with a separate syringe with the same needle just prior to the C.
-The itch, the irritability, the pain, the vomiting of chicken pox measles and mumps was assuaged in one hour with this last dose. Crusting of chicken pox was present in 5 hours instead of 7-9 days. 250 mg per kilogram eliminated the disease in contrast to the 65 mg which just suppressed it. 350 mg per kilogram may be employed along with antibiotics in treating stubborn bacterial infections. Because a virus infection will deplete the Vitamin C reserve, bleeding from the nose or chest would indicate an emergency situation; Vitamin C, using the above noted dosage schedule, should be pumped in immediately.
-For a very severe illness, the dose he used was large and the most effective route was intravenous, but the intramuscular route was satisfactory. He gave at least 350 mg per kilogram of body weight. (A 70 kg man is 150 pounds; thus 70 x 350= 24,500 mg. He would use a 25 gram dose for a 25 gram illness.) This amount was put in 500 cc of sterile water, usually with dextrose, saline or Ringer’s solution. It was diluted so that there was at least 18 cc of diluent to each gram of C. In small children, 2 or 3 grams can be given intramuscularly once every two hours. An ice cap to the buttocks will prevent soreness and induration. As much as 12 grams can be given in this manner into 2 or 3 different muscle sites with a 50 cc syringe; larger amounts must be diluted with dextrose or saline and run in by I.V. drip. If big concentrated doses are given by push (25 grams in a 100 cc syringe), the brain may become dehydrated causing convulsive movements of the legs. Intramuscular injections are always 500 mg to 1 cc solution. At least one gram of calcium gluconate must be added to the fluids each day. Massive doses of C pull calcium ions from platelets; and the clotting mechanism is weakened. Nosebleeds may occur. One gram of calcium gluconate is added to control acidity and to replace the calcium ion loss
-Sodium ascorbate is less painful. Some of us will put procaine, 2%, with the Vitamin C when injected into the muscle. Vitamin C can also be taken orally once the patient is recovering.
-This dose is repeated every hour for 6 to 12 times and then every 2-4 hours until recovery.
-If using under 400 mg per kg body weight, it can be given with the sodium salt. Doses over 400 mg per kg of body weight must be diluted to at least one gram to 18 cc of solution.
-He suggests the following for each bottle: 60 grams of C, 500 mg thiamin HCl, 300 mg pyridoxine, 400 mg calcium pantothenate, 100 mg riboflavin, 300 mg niacinamide. It is to be given once or twice daily.
-He used a 23 gauge needle intravenously and a 22 gauge needle for intramuscular use—one inch long for children and one and a half inch for adults.
-The idea of these big doses is to saturate the tissues; the white blood cells will be able to destroy pathogens. “I have seen diphtheria, hemolytic streptococcus infections clear within hours following an injection of ascorbic acid in a dose ranging from 500-700 mg per kilogram of body weight given intravenously as fast as the patient’s cardiovascular system will allow.”
-He got to know the vulnerability of viruses so well, he played games with them. “When proper amounts are used it will destroy all virus organisms.” He could give one gram of ascorbic acid every four hours and modify the disease symptoms, but if he gave one gram every two hours by mouth for four days, he had stopped the disease, apparently by killing the virus. If he gave this dose for only two days, the symptoms returned. (He kept measles simmering in his own children for a month by giving this dose for two days, then off for two then on, etc. I guess it was to help them develop immunity!)
-With 350 mg per kilogram of body weight every two hours, he could stop measles and dry up chicken pox. If he could get in the vein, 400 mg per kilogram two to three times in 24 hours was all that was required (he published this way back in 1951, in the Southern Medical Surgical Journal).
-This case demonstrates the usual quick response to therapy, but also the recurrence rate if the vitamin C is discontinued prematurely. The patient, a 73 year-old male, was admitted three times in 24 days with the same disease. He had a slight cold for a few days. Then abruptly, a severe headache was followed by a chill and coma. T=103, p=138, resp.=36, BP=150/90, white blood count was 10,000. Moisture was detected in his lungs. Muscle jerks appeared. Nasal oxygen begun. Intravenous achromycin and Vitamin C were begun; 20 grams of C was added to 378 cc of 5% dextrose in water. It was repeated in eight hours. He became conscious in 18 hours. He went home on the third day but returned in two weeks with the same findings and received the same treatment and sent home. In seven days he was back with the same symptoms. He was given 24 grams of C and sent home on achromycin and ten grams of C daily indefinitely. This case shows Dr. Klenner was confident that the C would handle the virus, but he needed the antibiotics to control the bacterial secondary invaders.
-The initial dose administered by needle is no less than 250 mg per kilogram of body weight. For children the dose would be two to three grams intramuscularly using a concentration of 500 mg per cc. Ice on the muscle after injection will usually control pain. “Massive use of C is compatible with any other drug and in most instances it will enhance the value of these other remedies.”
-As published in The Tri-State Medical Journal, February, 1960, he warned that “every cold must be considered as a probable source of brain pathology.” Most doctors are not impressed with the seriousness of the runny nose, the sore windpipe and the dry cough until this smoldering virus bursts through the defenses and attacks the brain.
-His routine for Virus Pneumonia was of 1000 mg of Vitamin C intravenously every six to twelve hours for a mild case. In children, 500 mg of C intramuscularly every six to twelve hours was about right. Three to seven injections were all that was required for complete clinical and X-ray resolution. Most patients felt better in just one hour and definite improvement after two hours. Nausea and headache disappeared after the first shot. Fever fell at least two degrees Fahrenheit in several hours after the first injection.
-He gave alkaline drinks as this impedes the excretion of the C through the kidneys. Mustard plasters were used to relieve chest pain and constricted breathing. In some patients cyanosis (blueness due to lack of oxygen in tissues) was immediately relieved by an additional injection of 500 mg of C.
-For poliomyelitis, he arbitrarily adopted the following routine injection schedule: 1000 to 2000 mg initially depending upon age. The intramuscular route was used for children under age four years. If the fever dropped in two hours, two more hours was allowed before the second dose. After 24 hours, if the fever remained down, this same dose was given every six hours for the next 48 hours. All sixty cases were well in 72 hours. Three however, had a relapse, so the C was continued in all 60 cases for another two days every eight to twelve hours. Home treatment was 2000 mg injected every six hours plus 1000 to 2000 mg orally every two hours. Two of the 60 patients had throat muscle paralysis and needed oxygen and drainage but were recovering in 36 hours.
-It is known that virus infections deplete the Vitamin C content of the adrenals.
-Vitamin C works as a destroyer of the virus but also as a safe and potent dehydrator and diuretic. (Most patients complain of thirst after an I.V. of ascorbic acid.)
-Dr. Klenner felt the best time to treat the virus was during the viremia stage; that is, when it was floating about in the blood stream and had not invaded the tissues. He repeats: “For optimum results the vitamin must be given in massive doses, every two to four hours, around the clock.” Intestinal absorption is inconsistent; it must be given by needle.
-In 1956 Dr. Klenner published, “Poliomyelitis—Case Histories” (Tri-State Medical Journal, Sept). He had a continuing supply of zingers he would throw at doctors who insisted on disregarding his logic. He quotes Ratner, “There are two ways of practicing the medical art: the first is to employ art; the second is to employ fancy.” If one has used speculation, preconceived opinions and prejudice, then he is proceeding by emotions, faith and dreams. We must proceed by REASON. Husky put it, “Science commits suicide when it adopts a creed.”
-For viral hepatitis, he said that vitamin C will cure it in two to four days. (500-700 mg/kg body weight taken orally; approximately 30 grams/24 hours). Dr. Klenner reports that Dr. Bauer at the University Clinic at Basel, Switzerland used just ten grams daily intravenously. It proved to be the best treatment available. He indicated that hepatitis (infectious and serum) can be reversed in a few days using intravenous Vitamin C.
–Case history of viral hepatitis: A 27 year old male with 103° temperature, nausea and jaundice of three days. 60 grams of sodium ascorbate in 600 cc of normal saline was given intravenously at 120 drops/minute. Five grams of Vitamin C was given orally every four hours around the clock. Fifteen grams of C was again given three hours after the first I.V. Another 60 grams of C was given intravenously twelve hours after the initial one (he used 5% glucose in water this time). That one took 75 minutes to accomplish. Then another fifteen grams of C intravenously after two more hours. For the 30 hours of treatment he received 270 grams intravenously and 45 grams orally—no diarrhea. Temperature was normal at this time and urine clear of bile. Discharged from the hospital, he was back to work. C sets in as a flash oxidizer and helps the body manufacture interferon, a natural antiviral agent.
–Case history of viral hepatitis: A 22 year old male with chills and fever and a diagnosis of viral hepatitis. His roommate had been admitted the day before. Fifteen grams of sodium ascorbate was given intravenously every twelve hours for three days, then once daily for six days. Sodium ascorbate was swallowed at five grams every four hours (135 grams intravenously, and 180 grams orally). No diarrhea appeared with these doses. He was sent home on the sixth day with no fever and no bile in the urine. Soon he was back to work. His roommate with just bed rest was in the hospital for 26 days!
-A 42-year-old male suffering from chronic hepatitis had been unsuccessfully treated with steroids for seven months. He was given B complex and Vitamin C: 45 grams of sodium ascorbate plus one gram of calcium gluconate in 500 cc of water with 5% glucose was given intravenously three times a week. He took five grams of C orally every four hours. He was free of the disease in five months. Dr. Klenner felt if he had more massive and continuous doses in the hospital he would have been well in a few weeks, but his peers on the staff would have denied the patient this safe treatment.
-Dr. Klenner reemphasized the point, “Sodium ascorbate in amounts ranging up to 900 mg per kilogram body weight every eight to twelve hours will effect cures in two to four days.”
-He felt that the risk of serum hepatitis from dialysis machines could be eliminated by flushing the machines with 50 grams of sodium ascorbate. When he needed to give a patient a blood transfusion he always added ten grams of sodium ascorbate to each pint. The Japanese, he said, have added but five grams of C to each unit of blood; result, no hepatitis and in thousands of cases.
–Fever blisters: three percent ointment of Vitamin C applied to the lips ten to fifteen times a day in a water soluble base speeds up the cure. A three-percent solution of ascorbic acid used as a douche will heal a cervical erosion; direct application of this solution by the physician would be prudent. Twenty grams of C orally each day would “erase this form of malignancy.” Dr. Klenner points out that the cancer seems to hit those with a hereditary tendency; a virus grows more eagerly in the susceptible. If there is a family tendency, oral C in large doses as a preventative makes sense.
-One to three injections of 400 mg per kg every eight hours will dry up chicken pox in 24 hours. Controls nausea with one gram of C per five cc of fluid. Thirst is precluded if a glass of juice is drunk just before the I.V.
-A ten month old baby had the high fever, watery nose, dry cough, the red eyes, and the Koplik spots that gave the disease away: hard measles. He gave 1000 mg of C every four hours. After twelve hours the temperature had fallen to 97.5°; the cough had stopped and the redness of the membranes had cleared. Just to see if this improvement happened to be the natural course of the disease, he stopped the C for just eight hours. The fever rose to 103.4°. The C injections were resumed and the fever dropped in a few hours to 99°. 1000 mg was given every four hours; no rash developed.
-An eight-year-old developed measles and mumps closely followed by encephalitis (T-104°). He could not eat, was stuporous and responded only to pain. Two hours after one injection of 2000 mg of Vitamin C, he sat up, ate a hearty meal and then played. In six hours he started to revert to his previous stupor, and the fever returned. Twelve hours after a second injection of two grams, and 1000 mg every two hours by mouth, he recovered. Dr. Klenner said, “The rude irritability shown prior to the first injection of Vitamin C was strikingly absent.” I think what he wants the reader to grasp is that the symptoms of these devastating virus diseases are similar to the clues seen in scorbutic patients.
-He reports cases of influenza, encephalitis, and measles easily cured with Vitamin C injections and oral doses. A 23-year-old male developed mumps plus bilateral orchitis; his fever was 105°, and he was in overwhelming pain with “testicles the size of tennis balls.” After one 1000-mg injection of Vitamin C intravenously the pain began to subside and after six more shots spaced every two hours the pain was gone. The fever was normal in 36 hours. He was up, about and well in 60 hours. Total dose 25,000 mg.
-Dr. Klenner felt mono is related to cancer because the same virus (Epstein-Barr) is found in Burkitt’s lymphoma. The disease, mono, can be eliminated with an I.V. of C in just a few days, “The actual time being directly proportional to the amount of the vitamin employed in relation to the severity of the infection.” (Most use Dr. Cathcart’s formula for the amount of C to be given: “I think this is a 50 gram disease: some fever, generalized aches, but ambulatory.”) In one patient who was given the last rites by her church, the girl’s mother took things into her own hands when the attending physician refused to give ascorbic acid. In each bottle of I.V. fluid she would secretly and quickly “tap in” 20 -30 grams of Vitamin C. The patient made an uneventful recovery. Her mother has her BS in nursing and has been a long time advocate of massive “C” therapy. (100 gram disease: 102-103°, holding down fluids but needs to stay in bed, miserable. 200 gram disease: 104 degree temperature, semi-comatose, somewhat dehydrated; hospitalization a good idea.)
–Pancreatitis. He treated but one case of this. He put 60 grams of sodium ascorbate in 1000 cc of 5% dextrose in water and let it drip in rapidly and the patient was able to go home in twelve hours.
–Rocky Mountain Spotted Fever. Dr. Klenner was an authority in the treatment of this rather debilitating, serious disease because his practice was right in the middle of a constant locus of infection for tick bite fever. Dr. Klenner had been taught in his training that there was no cure for it, only supportive. So when he was confronted with an obvious case—104.4° degree temperature, spots over body, coma, and positive blood test—he quickly gave 30 grams of C intravenously every six hours. The patient was given para-aminobenzoic acid orally, six grams, every two hours x3, then 4 grams every two hours for 24 hours, then 4 grams every 4 hours until his fever was gone for 24 hours. At about the sixth hour of treatment he became conscious and rational. He was sent home on the sixth day, fully recovered. The C is given around the clock and at the 500-900 mg per kg body weight level. The disease “can always be reversed.”
-Dr. Klenner reports on other research: Vitamin C inactivates the toxin of tetanus. He felt that the number of fatalities from the disease were equal to the number of those who die from the treatment. He emphasized some principles of treatment 30 to 40 years ago that many of us have forgotten: namely, do no harm, and the body has tremendous restorative powers if the doctor will supply it with the raw materials to promote recovery.
–Chronic cystitis is usually associated with alkaline urine. Germs grow more easily in this alkaline urine. Vitamin C will discourage these bacteria and cut the chance of an ascending infection which might devastate the kidneys (pyelitis). Ten grams of C per day are suggested.
-For acute alcoholism Dr. Klenner has given 1000 mg of thiamin intramuscularly every two hours until recovery. Pyridoxine, 500 mg is given every six hours. 40 grams of C intravenously will detoxify the patient.
–Arthritis: Vitamin C counteracts the damaging effects of aspirin. C is the number one precursor for collagen formation. If serum levels of C are high, synovial fluid is thinner allowing for easier joint movement. Those taking 15 to 25 grams daily will experience commensurate benefit. Prevention seems prudent. “A person who will take ten to twenty grams of ascorbic acid a day along with other nutrients might very well never develop arthritis.”
–Cancer: He cites Schlegel’s (Tulane University) use of ascorbic acid (1.5 grams a day only) in preventing bladder cancer recurrence. “This is the so called wasted Vitamin C.” He “demonstrated that in the presence of ascorbic acid, carcinogenic metabolites will not develop in the urine. They suggested that spontaneous tumor formation is the result of faulty tryptophan metabolism while urine is retained in the bladder.” Other researchers report that the depletion of mast cells from guinea pig skin was due to ascorbic acid deficiency. It suggests Vitamin C is necessary for the formation and maintenance of mast cells. Vitamin C will control myelocytic leukemia with 25-30 grams orally daily. “How long must we wait for someone to start continuous ascorbic acid drip for two to three months, giving 100 to 300 grams each day, for various malignant conditions?
–Small basal cell epithelioma: 30% Vitamin C ointment.
-His protocol for treating cancer is printed here in total. All of this is designed to kill the cancer cells by shoring up the immune system.
[Note: Back then there was less industrial pollution, no GMOs and less toxicity in general. The dietary guidelines in this diet make no sense in that they contain too much sugar and protein. A ketogenic diet is the one thing that is showing differences for cancer patients nowadays. For more info see Ketogenic diet may be key to cancer recovery.]
He reported a case of a man with lymph glands all over his body. He got the above treatment and although the glands increased in size for a while, his liver and spleen were back to normal size in four months. Dr. Klenner noticed a ‘parachute-like’ substance in the urine. Microscopic examination revealed they were clumps of cancer cells.
Another case was that of a woman who had an adenocarcinoma of two years duration. She had had chemotherapy, two surgeries and extensive radiation over her chest, especially the neck area where the cancerous glands were. The cancer had spread to her lungs, her abdomen and six glands in her neck. Dr. Klenner gave her the above protocol. In three months the lesion in her lung had cleared and gone were the glands in her neck. After six months of intravenous Vitamin C and the B complex, the abdominal masses had disappeared, but she could not swallow food. The radiation had scarred her esophagus beyond dilatation and she refused more surgery. The cancer was gone; she died from starvation due to the radiation.
Dr Klenner summarized this paper with this: “The results suggest that larger daily amounts could be given in a hospital with faster results. I would suggest at least 100 grams in 1000 cc of fluid and given every twelve to 24 hours. The vitamins and the calcium gluconate also must be given.” He thought interferon could be assayed while the patient is in the hospital. “How long will it take for the general population to challenge the drug cartel?”
-There is a relationship of Vitamin C and cholesterol. Scorbutic guinea pigs have high cholesterol levels. Way back in 1947 high intravenous doses of Vitamin C were found effective in lowering cholesterol levels. Cholesterol levels in the blood of subjects vary with the amount of C used. In one patient the cholesterol was lowered 42 mg percent in six weeks when his oral intake of Vitamin C was increased from 10 grams a day to 20 grams a day. Extra C seems to be critical especially in those with a family tendency. [And as long as there is no excess iron in the body, cholesterol itself will be less likely to be toxic]
–Cavities: A gram of Vitamin C every day for each year of life (five grams a day for the five year old) will prevent cavities. Ten grams a day from age ten years for a lifetime should maintain that advantage.
–Disc, ruptured intervertebral: will be prevented with the ten-grams-a-day dose. Adequate amounts seem necessary for disc metabolism and maintenance.
-Corneal ulcers: healed with but 1.5 grams of C daily. The pain of a corneal burn was relieved immediately with twelve grams of C intravenously. The cornea was normal in 24 hours.
-He reported the story of a seven year old diabetic, who developed measles, and his insulin requirements went from 5 units to more than 90 units a day, but with one gram of Vitamin C every four hours his infection and elevated blood sugar came under control. In these diabetic cases, the Vitamin C can be cut back to reasonable levels after the infection is under control. Large prolonged doses of “Vitamin C might prove undesirable due to its dehydrating and diuretic powers.”
-As a matter of fact Dr. Klenner had been studying the effects of ten grams of C per day orally in patients with diabetes mellitus; 60% were able to control the condition with diet and C. The other 40% were able to reduce the insulin dose. Wounds healed more readily.
–Glaucoma: patients use 35 grams of C (100 mg/kg after meals and bedtime) in divided doses during the 24 hours and this osmotic dehydration of the eyeball was safe and effective. “The size of the dose does make a difference—a real difference.”
–Schizophrenia: Dr. Klenner reminds us of Hoffer and Osmond’s work with niacin and Vitamin C back in the early 1950’s. Six to 8 grams of C a day made the niacin work. One schizophrenic took one gram every hour for 48 hours and was completely recovered for six months with no further treatment. These megadoses halved the suicide rate. It has been demonstrated that schizophrenics burn up C ten times faster than the normal population.
–Burns: can be treated with Vitamin C. “30-100 grams of Vitamin C is the proper amount to employ.” (500 mg per kg of body weight diluted to at least 18 cc per gram of C using 5% dextrose or saline in water or Ringer’s solution, repeated every eight hours for several days, then at twelve hour intervals. Calcium gluconate is added.) “Vitamin C is given until healing takes place.” It takes seven to thirty days depending upon the degree of the burn. It may prevent the need for grafting as it keeps the tissues oxygenated thus preventing the blood from sludging. [Kniseley] On the fourth to fifth day the malodorous burn eschars will fall off leaving normal tissue. Vitamin C also eliminates pain; opiates are less necessary. (It stimulates endorphin production in the brain.) Three percent ascorbic acid solution is used as a spray every two to four hours for five days. Pseudomonas: (a nasty bacteria, often seen in burn patients; very resistant to antibiotics): three percent spray plus massive injections.
–Heat stroke: 500 mg per kg of body weight will reverse it.
–Sunburn: One gram taken every one to two hours during exposure will prevent sunburn; an I.V. injection will quickly relieve the pain and erythema. Even second-degree burns will be healed.
-Prickly heat, heat stroke, heat collapse can all be treated; the latter needs twelve to forty grams intravenously. Electric shock patients must be given Vitamin C immediately after the accident—including lightning victims.
-Vitamin C will control the side effects of radiation including radiation burns. “Who can say what 100 to 300 grams given intravenously daily for several months might accomplish in cancer? The potential is so great and the employment so elementary that only the illiterate will continue to deny its use.”
–Surgery: Way back in 1960 and again in 1966, Dr. Klenner delivered papers before the Tri-State Medical Society calling attention to the “scurvy levels” of C in post-operative patients. The levels began to fall six hours after surgery and by 24 hours the levels were 3/4 lower than pre-op. Tensile strength of healing wounds is lowered if the plasma drops to scurvy levels. The lower the C levels the poorer the wound heals. Even as little a dose as 500 mg of C orally “was remarkable successful in preventing shock and weakness,” following dental extraction.
-Dr. Klenner used 10 grams preoperatively intravenously and ten grams in each post-operative bottle and then ten grams orally when eating was resumed. Surgical wounds rarely separated with this method. Fractures healed faster. (Some surgeons will give ten grams of Vitamin C at the end of the operation, and the patient is awake and alert in 60 seconds. No need for the nausea and vomiting in the recovery room.)
–Heavy Metal Poisonings: Especially lead and mercury—are controlled with Vitamin C injections and oral intake. An intake of Vitamin C daily will protect animals—and by extrapolation, humans—from fatal doses of mercury. If a guinea pig needed 200 mg one day to protect it from an otherwise fatal dose of mercury, the human would need 14 grams daily. Smaller doses would be able to protect the body from smaller amounts of the toxin.
-Lead poisoning: 350 mg of Vitamin C per one kg of body weight taken intramuscularly every two to four hours; recovery in less than 72 hours.
-Dr. Klenner found that the amount of C used “in any case is the all important factor. In 28 years of research we have observed that 30 grams each day is critical in terms of response” regardless of age and weight. (Barbiturate intoxication, snake bite and viral encephalitis may require larger doses in some individuals.)
–Carbon Monoxide (CO): if 12 to 50 grams of Vitamin C is injected rapidly into the blood stream, it acts as an oxidizer and will “pull CO from hemoglobin to form carbon dioxide” which is easily exhaled. A burn victim should immediately receive a dose of 500 mg of C per kg of body weight intravenously. It will “neutralize the CO or smoke poisoning while at the same time it will prevent blood sludging which in the major factor in the development of third degree burns.” An accidental carbon monoxide poisoning was reversed in ten minutes with 12 grams of ascorbic acid in a 50 cc syringe using a twenty gauge needle. (”We employ a twenty-gauge needle when using a 50 cc syringe; a twenty-one gauge for a thirty-cc syringe, a twenty-two gauge for a twenty cc syringe and a twenty-three gauge needle for a ten cc syringe“).
-In another Tri-State Medical Journal of December, 1957, he outlined the physiology and treatment of Black Widow Spider poisoning in a case history. Some of those bitten are not affected at all because the spider was out of poison, but some can be devastated and may die, partly because of poor resistance but also due to the quantity injected. It can be confused with pancreatitis, renal colic, food poisoning, tetanus, angina, bowel obstruction, pneumonia, perforated ulcer. The abdominal wall muscles become rigid, the victims have cold sweat, their temperature and blood pressure shoot up, they vomit, have muscle twitches and spasms, cyanosis, chills, convulsions and delirium. The painful muscle spasms occur within minutes of the original bite. The cramps occur in all the large muscles of the body; the victims roll and toss and moan in agony. Until someone used calcium gluconate, there were 90 ineffective treatments. An anti-venom is on the market, but severe reactions and even death have been attributed to its use. The treatment Dr. Klenner suggests is his friend, Vitamin C, 350 mg per kg of body weight intravenously along with calcium gluconate. His three and a half year old patient had been getting worse for 24 hours with abdominal cramps which the parents assumed were due to food poisoning. She became quieter, feverish, constipated and her abdomen was exquisitely tender. She was becoming stuporous. Dr Klenner noted the red, swollen area around her naval, and two tiny spots about one eighth of an inch apart were noted in the middle: the fang marks of a Black Widow Spider. He gave one gram of calcium gluconate and 4 grams of Vitamin C intravenously. In 6 hours she was more responsive, and her temperature had dropped from 103 degrees to 101 degrees and she was given another four grams I.V. “Some ascorbic acid behaves much like calcium in the body, and also acts synergistically with it, we elected to observe its action.” The child was destined to die. “Some physicians would stand by and see their patient die rather than use ascorbic acid because in their finite minds it exists only as a vitamin.”
-Dr. Klenner was very confident about the benefits of intravenous Vitamin C to treat the poisonous effects of insects and reptiles,. He felt all emergency rooms should be adequately stocked. He used sodium ascorbate, 7.5 grams in 30 ml. The syringes are 5 to 60 cc. The needles are 20 gauge (big), one inch long to 31 gauge (I have trouble believing this) one inch long. I get “miracle like responses.”
-“Sodium ascorbate will cure any type of snake bite.” The amounts and the speed of injection are critical. Forty to 60 grams intravenously as a starter. Klenner cites the 6500 deaths a year from snake bites, but many more from insects, bees, spider, plants and some caterpillars. They produce formic acid, histamine and specific toxin albumins. Some are neurotoxins; some cause capillary damage and hemorrhage. When cells are damaged proteins are deaminized, producing histamine and other toxic products; shock may occur. These deaminizing enzymes from the damaged cells are inhibited by Vitamin C. The pH of cells changes when cells are damaged; enzymes become destructive instead of constructive. C reverses this. Vitamin C is reduced in the serum of those in shock. 350-700 mg per kg body weight is the saving intravenous dose. In children up to two grams can be given in each of several areas (a twenty kg five year old could get two grams in each of four sites. Ice before and after the injection would control the pain).
–Multiple Sclerosis & Myasthenia Gravis. Adequate oxygen is assured if the lungs and hemoglobin are normal, but also by taking 10 to 30 grams of ascorbic acid by mouth every 24 hours. Oxygen is released for tissue use when ascorbic acid becomes dehydroascorbic acid. Enzymes are necessary to make all these reactions possible. Genetic faults manifest themselves through enzymatic deficiencies. He puts Myasthenia Gravis and Multiple Sclerosis in the same therapeutic group as he found thiamin was the key to the therapy. M.G. is a genetically transmitted disease and M.S. is triggered by a virus and mimics poliomyelitis. Nerve damage in M.S. is due to microscopic hemorrhages in the nervous system. During healing, scar tissue contracts clamping off capillary flow and nutrition. This wasting results in loss of the myelin sheath protection. He felt that remyelinating these damaged nerves was every bit as hopeful as the myelination that occurs normally in infancy with nothing more spectacular than breast milk. It requires two years of treatment to repair the damage caused by one year of the disease. He cites works in the late 1930s by Stern at Columbia University who used thiamin intraspinally for the treatment of Multiple Sclerosis with astonishing results. After 30 mg of thiamin was injected into the spinal canal of paralyzed MS. victims, they had a temporary remission. Dr. Klenner felt that most cases (80%) of Multiple Sclerosis had their origin in an illness—probably a coxsackie virus—compatible with a summer “flu”. He mentioned other theories of the etiology of M.S., but was convinced that the scar tissue that forms around the nerves and produces the symptoms “is the end result of microscopic hemorrhages following virus invasion.”
-Dr. Klenner reports on a few minor complications. Some diarrhea might have been due to sodium bisulfite. Induration after intramuscular injections was found to be due to the Vitamin C not being injected deeply enough into the muscle. (One had to be drained—a sterile abscess.) If the concentration was one gram to 5 cc it caused a vein spasm up the arm from the injection site in three cases. A thrombosis of the vein occurred in but one case. A minor face rash developed in a few that cleared after the C was stopped. Calcium seemed to enhance the effects of the C when both were give simultaneously. But a gram of just the calcium given intravenously can slow the heart rate to a dangerous degree.
-Oxalic acid precipitates out of solution only from a neutral or alkaline solution—pH 7 to pH 10. Urine pH in those consuming ten grams of Vitamin C daily is about 6. Even in diabetics who take this large amount of C (10 grams), the urinary oxalate excretion remains relatively unchanged. “Vitamin C is an excellent diuretic. No urinary stasis; no urine concentration. The ascorbic acid/kidney stone story is a myth.” One more bon mot: “Methylene will dissolve calcium oxalate stones, if the patient is given 65 mg orally two to three times a day,” he learned from Medical World News (Smith, M.J.V., M.D.: Dec. 4, 1970). (90% of all stones are calcium stones. Calcium is soluble in acid media. Vitamin C acidifies the urine. Acid urine discourages the growth of bacteria. Although uric acid stones are theoretically possible with high doses of C and a low urinary pH, none have been reported.)
-He reiterates the safety of large doses of C. He states that plasma doses of greater than twenty times normal produce no ill effects. Diarrhea is the most common side effect of large doses. Some notice thickening of subcutaneous tissue is the C is not injected deeply enough into, the muscle. (That induration will eventually resolve.) Some will complain of venous irritation and spasm if the intravenous Vitamin C is too concentrated or too rapidly injected. (C mixed with calcium will reduce this irritation.) A rare thrombosis may occur if the concentration of the C is greater than 500 mg per cc. Some will faint if the injection is given too rapidly. (It is best to have the patient lie flat.) Large doses by mouth may cause a genital or anal rash and itch. He also showed how safe large doses of C were. He gave 200 patients 500 to 1000 mg of C every four to six hours for five to ten days. No laboratory abnormalities were found in blood or urine and no symptoms were noted except one percent who developed vomiting; he assumed from a hypersensitive stomach. And these patients had no virus infection to “assist in destroying the vitamin.”
Current IV Vitamin C Guidelines
Nowadays baseline blood tests include screening for red blood cell glucose-6-phospahte dehydrogenase deficiency. Those with G6PD, an extremely rare condition, can have problems of hemolysis when vitamin C at large doses are first infused.
In case of iron overload, vitamin C is also discouraged as it will increase iron’s absorption, often carrying its toxic effect into the heart. Due to iron overload’s pro-cancer and pro-disease effects, many people will find themselves not able to benefit from vitamin C. These people will only recover their health and energy with iron chelation therapies such as EDTA and bloodletting. Yes, donating blood can be very good for your health!
There are numerous case histories where vitamin C’s anti-cancer properties have been reported. You’ll find resources on where these therapies are performed at Orthomolecular.org.
Usually a protocol will look like this:
Week 1: 1 x 15 g infusion per day, 2-3 per week.Week 2: 1 x 30 g infusion per day, 2-3 per week.
Week 3: 1 x 65 g infusion per day, 2-3 per week.
The dose is then adjusted to achieve blood concentrations of 400mg/dL, 2-3 infusions per week. Sodium ascorbate is the one usually used for IV vitamin C infusion, as it is more friendly.
Lots of folks just do their own liposomal vitamin C and voilà.
[Snipped the part on oral doses. Very important info though!]
Clinical Guide to the Use of Vitamin C by Lendon H. Smith, M.D.
These are the Clinical Experiences of Frederick R. Klenner, M.D., as abbreviated, sumarized and annotated by
Lendon H. Smith, M.D.. You can read the full article here.
-The patient should “get large doses of Vitamin C in all pathological conditions while the physician ponders the diagnosis.”
-If we base our needs on the amounts other mammals manufacture with their intact enzyme it comes to 2-4 grams daily in the unstressed condition. Under stress 70 kg of rats make 15 grams of C.
-If you are hypoascorbemic because you cannot manufacture Vitamin C from sugar, extra glucose in your diet will not help, you need to take Vitamin C.
-Vitamin C level of the blood plasma fell to zero for 90 days before there was obvious clinical evidence and that this was as long as 132 days before the first signs appeared.
-As an oxidizing agent massive amounts, i.e., 5-150 grams, intravenously, for certain pathological conditions.
-Vitamin C acts as a reducing agent, an oxidizing agent, an anti-clotting agent, an antihistamine, and as an anti-infective agent.
-Ascorbic acid enters all cells. It “proceeds to take up the protein coats being manufactured by the virus nucleic acid, thus preventing the assembly of new virus units.”
-Failure to benefit from Vitamin C use is usually due to inadequate amounts being used for too short a period of time.
-Vitamin C combines directly with the toxin/virus. This new compound is oxidized by Vitamin C; the toxin/virus and the Vitamin C are destroyed. This must be why C has to be continued after the apparent cure.
-The anaerobic condition in the tissue is relieved. Acidity is decreased and large amounts of Adrenaline disappear. The constriction of the blood vessels ceases and the liver and pancreas can receive the proper nutrients to function. Properly calculated doses of C on a continuing basis will restore the normal physiology of the body.
-The adrenals and Vitamin C are interrelated.
-Patients ill with a virus would show petechial hemorrhages (small leaks of blood into the skin) when a tourniquet was applied to increase venous backpressure. Capillary weakness is a sign of low levels of Vitamin C.
-The collagen of all fibrous tissue structures is dependent on an adequate level of Vitamin C. These weak capillary walls may allow a simple virus to invade the brain
-Vitamin C acts as catalyst in the assimilation of iron.
A note of caution: Those with iron overload (ask your physician to test for ferritin, transferrin, TIBC and iron) should keep in mind that vitamin C increases the absorption of iron into the body, especially in the heart where it can cause heart failure, palpitations and others. Ferritin levels should be ideally less than 80 and transferrin saturation should be less than 40%. If you are above those levels, you might want to donate some blood or refer to the Iron Disorders Institute. A great book on the subject is The Elephant Iron by Roberta Crawford.
-Ascorbic acid is a necessary coenzyme in the metabolic oxidation of tyrosine. The latter is necessary to break down protein to a usable amino acid.
-Highly alkaline urine has less Vitamin C. The Vitamin C would be thus retained in the tissues helping to guard against the viruses and bacteria. When Vitamin C levels drop, glycogen in the liver is converted to glucose: a response to stress.
-The usual dose of 65 mg per kilogram of body weight may be expected to take care of the usual virus infection when given every 2-4 hours by needle. The more severe condition would respond to larger single injections.
-However “if the activity of the pathogen is completely stopped, the development of active immunity will be interrupted.” Therefore, modification of childhood diseases is the aim of Vitamin C treatment, not the complete overnight suppression that would prevent the body from making immune memory. To accomplish modification, 250 mg per kilogram should be given intramuscularly. If necessary, half of this amount would be given in eight hours. Procaine 1.5-2% can be given with a separate syringe with the same needle just prior to the C.
-The itch, the irritability, the pain, the vomiting of chicken pox measles and mumps was assuaged in one hour with this last dose. Crusting of chicken pox was present in 5 hours instead of 7-9 days. 250 mg per kilogram eliminated the disease in contrast to the 65 mg which just suppressed it. 350 mg per kilogram may be employed along with antibiotics in treating stubborn bacterial infections. Because a virus infection will deplete the Vitamin C reserve, bleeding from the nose or chest would indicate an emergency situation; Vitamin C, using the above noted dosage schedule, should be pumped in immediately.
-For a very severe illness, the dose he used was large and the most effective route was intravenous, but the intramuscular route was satisfactory. He gave at least 350 mg per kilogram of body weight. (A 70 kg man is 150 pounds; thus 70 x 350= 24,500 mg. He would use a 25 gram dose for a 25 gram illness.) This amount was put in 500 cc of sterile water, usually with dextrose, saline or Ringer’s solution. It was diluted so that there was at least 18 cc of diluent to each gram of C. In small children, 2 or 3 grams can be given intramuscularly once every two hours. An ice cap to the buttocks will prevent soreness and induration. As much as 12 grams can be given in this manner into 2 or 3 different muscle sites with a 50 cc syringe; larger amounts must be diluted with dextrose or saline and run in by I.V. drip. If big concentrated doses are given by push (25 grams in a 100 cc syringe), the brain may become dehydrated causing convulsive movements of the legs. Intramuscular injections are always 500 mg to 1 cc solution. At least one gram of calcium gluconate must be added to the fluids each day. Massive doses of C pull calcium ions from platelets; and the clotting mechanism is weakened. Nosebleeds may occur. One gram of calcium gluconate is added to control acidity and to replace the calcium ion loss
-Sodium ascorbate is less painful. Some of us will put procaine, 2%, with the Vitamin C when injected into the muscle. Vitamin C can also be taken orally once the patient is recovering.
-This dose is repeated every hour for 6 to 12 times and then every 2-4 hours until recovery.
-If using under 400 mg per kg body weight, it can be given with the sodium salt. Doses over 400 mg per kg of body weight must be diluted to at least one gram to 18 cc of solution.
-He suggests the following for each bottle: 60 grams of C, 500 mg thiamin HCl, 300 mg pyridoxine, 400 mg calcium pantothenate, 100 mg riboflavin, 300 mg niacinamide. It is to be given once or twice daily.
-He used a 23 gauge needle intravenously and a 22 gauge needle for intramuscular use—one inch long for children and one and a half inch for adults.
-The idea of these big doses is to saturate the tissues; the white blood cells will be able to destroy pathogens. “I have seen diphtheria, hemolytic streptococcus infections clear within hours following an injection of ascorbic acid in a dose ranging from 500-700 mg per kilogram of body weight given intravenously as fast as the patient’s cardiovascular system will allow.”
-He got to know the vulnerability of viruses so well, he played games with them. “When proper amounts are used it will destroy all virus organisms.” He could give one gram of ascorbic acid every four hours and modify the disease symptoms, but if he gave one gram every two hours by mouth for four days, he had stopped the disease, apparently by killing the virus. If he gave this dose for only two days, the symptoms returned. (He kept measles simmering in his own children for a month by giving this dose for two days, then off for two then on, etc. I guess it was to help them develop immunity!)
-With 350 mg per kilogram of body weight every two hours, he could stop measles and dry up chicken pox. If he could get in the vein, 400 mg per kilogram two to three times in 24 hours was all that was required (he published this way back in 1951, in the Southern Medical Surgical Journal).
-This case demonstrates the usual quick response to therapy, but also the recurrence rate if the vitamin C is discontinued prematurely. The patient, a 73 year-old male, was admitted three times in 24 days with the same disease. He had a slight cold for a few days. Then abruptly, a severe headache was followed by a chill and coma. T=103, p=138, resp.=36, BP=150/90, white blood count was 10,000. Moisture was detected in his lungs. Muscle jerks appeared. Nasal oxygen begun. Intravenous achromycin and Vitamin C were begun; 20 grams of C was added to 378 cc of 5% dextrose in water. It was repeated in eight hours. He became conscious in 18 hours. He went home on the third day but returned in two weeks with the same findings and received the same treatment and sent home. In seven days he was back with the same symptoms. He was given 24 grams of C and sent home on achromycin and ten grams of C daily indefinitely. This case shows Dr. Klenner was confident that the C would handle the virus, but he needed the antibiotics to control the bacterial secondary invaders.
-The initial dose administered by needle is no less than 250 mg per kilogram of body weight. For children the dose would be two to three grams intramuscularly using a concentration of 500 mg per cc. Ice on the muscle after injection will usually control pain. “Massive use of C is compatible with any other drug and in most instances it will enhance the value of these other remedies.”
-As published in The Tri-State Medical Journal, February, 1960, he warned that “every cold must be considered as a probable source of brain pathology.” Most doctors are not impressed with the seriousness of the runny nose, the sore windpipe and the dry cough until this smoldering virus bursts through the defenses and attacks the brain.
-His routine for Virus Pneumonia was of 1000 mg of Vitamin C intravenously every six to twelve hours for a mild case. In children, 500 mg of C intramuscularly every six to twelve hours was about right. Three to seven injections were all that was required for complete clinical and X-ray resolution. Most patients felt better in just one hour and definite improvement after two hours. Nausea and headache disappeared after the first shot. Fever fell at least two degrees Fahrenheit in several hours after the first injection.
-He gave alkaline drinks as this impedes the excretion of the C through the kidneys. Mustard plasters were used to relieve chest pain and constricted breathing. In some patients cyanosis (blueness due to lack of oxygen in tissues) was immediately relieved by an additional injection of 500 mg of C.
-For poliomyelitis, he arbitrarily adopted the following routine injection schedule: 1000 to 2000 mg initially depending upon age. The intramuscular route was used for children under age four years. If the fever dropped in two hours, two more hours was allowed before the second dose. After 24 hours, if the fever remained down, this same dose was given every six hours for the next 48 hours. All sixty cases were well in 72 hours. Three however, had a relapse, so the C was continued in all 60 cases for another two days every eight to twelve hours. Home treatment was 2000 mg injected every six hours plus 1000 to 2000 mg orally every two hours. Two of the 60 patients had throat muscle paralysis and needed oxygen and drainage but were recovering in 36 hours.
-It is known that virus infections deplete the Vitamin C content of the adrenals.
-Vitamin C works as a destroyer of the virus but also as a safe and potent dehydrator and diuretic. (Most patients complain of thirst after an I.V. of ascorbic acid.)
-Dr. Klenner felt the best time to treat the virus was during the viremia stage; that is, when it was floating about in the blood stream and had not invaded the tissues. He repeats: “For optimum results the vitamin must be given in massive doses, every two to four hours, around the clock.” Intestinal absorption is inconsistent; it must be given by needle.
-In 1956 Dr. Klenner published, “Poliomyelitis—Case Histories” (Tri-State Medical Journal, Sept). He had a continuing supply of zingers he would throw at doctors who insisted on disregarding his logic. He quotes Ratner, “There are two ways of practicing the medical art: the first is to employ art; the second is to employ fancy.” If one has used speculation, preconceived opinions and prejudice, then he is proceeding by emotions, faith and dreams. We must proceed by REASON. Husky put it, “Science commits suicide when it adopts a creed.”
-For viral hepatitis, he said that vitamin C will cure it in two to four days. (500-700 mg/kg body weight taken orally; approximately 30 grams/24 hours). Dr. Klenner reports that Dr. Bauer at the University Clinic at Basel, Switzerland used just ten grams daily intravenously. It proved to be the best treatment available. He indicated that hepatitis (infectious and serum) can be reversed in a few days using intravenous Vitamin C.
–Case history of viral hepatitis: A 27 year old male with 103° temperature, nausea and jaundice of three days. 60 grams of sodium ascorbate in 600 cc of normal saline was given intravenously at 120 drops/minute. Five grams of Vitamin C was given orally every four hours around the clock. Fifteen grams of C was again given three hours after the first I.V. Another 60 grams of C was given intravenously twelve hours after the initial one (he used 5% glucose in water this time). That one took 75 minutes to accomplish. Then another fifteen grams of C intravenously after two more hours. For the 30 hours of treatment he received 270 grams intravenously and 45 grams orally—no diarrhea. Temperature was normal at this time and urine clear of bile. Discharged from the hospital, he was back to work. C sets in as a flash oxidizer and helps the body manufacture interferon, a natural antiviral agent.
–Case history of viral hepatitis: A 22 year old male with chills and fever and a diagnosis of viral hepatitis. His roommate had been admitted the day before. Fifteen grams of sodium ascorbate was given intravenously every twelve hours for three days, then once daily for six days. Sodium ascorbate was swallowed at five grams every four hours (135 grams intravenously, and 180 grams orally). No diarrhea appeared with these doses. He was sent home on the sixth day with no fever and no bile in the urine. Soon he was back to work. His roommate with just bed rest was in the hospital for 26 days!
-A 42-year-old male suffering from chronic hepatitis had been unsuccessfully treated with steroids for seven months. He was given B complex and Vitamin C: 45 grams of sodium ascorbate plus one gram of calcium gluconate in 500 cc of water with 5% glucose was given intravenously three times a week. He took five grams of C orally every four hours. He was free of the disease in five months. Dr. Klenner felt if he had more massive and continuous doses in the hospital he would have been well in a few weeks, but his peers on the staff would have denied the patient this safe treatment.
-Dr. Klenner reemphasized the point, “Sodium ascorbate in amounts ranging up to 900 mg per kilogram body weight every eight to twelve hours will effect cures in two to four days.”
-He felt that the risk of serum hepatitis from dialysis machines could be eliminated by flushing the machines with 50 grams of sodium ascorbate. When he needed to give a patient a blood transfusion he always added ten grams of sodium ascorbate to each pint. The Japanese, he said, have added but five grams of C to each unit of blood; result, no hepatitis and in thousands of cases.
–Fever blisters: three percent ointment of Vitamin C applied to the lips ten to fifteen times a day in a water soluble base speeds up the cure. A three-percent solution of ascorbic acid used as a douche will heal a cervical erosion; direct application of this solution by the physician would be prudent. Twenty grams of C orally each day would “erase this form of malignancy.” Dr. Klenner points out that the cancer seems to hit those with a hereditary tendency; a virus grows more eagerly in the susceptible. If there is a family tendency, oral C in large doses as a preventative makes sense.
-One to three injections of 400 mg per kg every eight hours will dry up chicken pox in 24 hours. Controls nausea with one gram of C per five cc of fluid. Thirst is precluded if a glass of juice is drunk just before the I.V.
-A ten month old baby had the high fever, watery nose, dry cough, the red eyes, and the Koplik spots that gave the disease away: hard measles. He gave 1000 mg of C every four hours. After twelve hours the temperature had fallen to 97.5°; the cough had stopped and the redness of the membranes had cleared. Just to see if this improvement happened to be the natural course of the disease, he stopped the C for just eight hours. The fever rose to 103.4°. The C injections were resumed and the fever dropped in a few hours to 99°. 1000 mg was given every four hours; no rash developed.
-An eight-year-old developed measles and mumps closely followed by encephalitis (T-104°). He could not eat, was stuporous and responded only to pain. Two hours after one injection of 2000 mg of Vitamin C, he sat up, ate a hearty meal and then played. In six hours he started to revert to his previous stupor, and the fever returned. Twelve hours after a second injection of two grams, and 1000 mg every two hours by mouth, he recovered. Dr. Klenner said, “The rude irritability shown prior to the first injection of Vitamin C was strikingly absent.” I think what he wants the reader to grasp is that the symptoms of these devastating virus diseases are similar to the clues seen in scorbutic patients.
-He reports cases of influenza, encephalitis, and measles easily cured with Vitamin C injections and oral doses. A 23-year-old male developed mumps plus bilateral orchitis; his fever was 105°, and he was in overwhelming pain with “testicles the size of tennis balls.” After one 1000-mg injection of Vitamin C intravenously the pain began to subside and after six more shots spaced every two hours the pain was gone. The fever was normal in 36 hours. He was up, about and well in 60 hours. Total dose 25,000 mg.
-Dr. Klenner felt mono is related to cancer because the same virus (Epstein-Barr) is found in Burkitt’s lymphoma. The disease, mono, can be eliminated with an I.V. of C in just a few days, “The actual time being directly proportional to the amount of the vitamin employed in relation to the severity of the infection.” (Most use Dr. Cathcart’s formula for the amount of C to be given: “I think this is a 50 gram disease: some fever, generalized aches, but ambulatory.”) In one patient who was given the last rites by her church, the girl’s mother took things into her own hands when the attending physician refused to give ascorbic acid. In each bottle of I.V. fluid she would secretly and quickly “tap in” 20 -30 grams of Vitamin C. The patient made an uneventful recovery. Her mother has her BS in nursing and has been a long time advocate of massive “C” therapy. (100 gram disease: 102-103°, holding down fluids but needs to stay in bed, miserable. 200 gram disease: 104 degree temperature, semi-comatose, somewhat dehydrated; hospitalization a good idea.)
–Pancreatitis. He treated but one case of this. He put 60 grams of sodium ascorbate in 1000 cc of 5% dextrose in water and let it drip in rapidly and the patient was able to go home in twelve hours.
–Rocky Mountain Spotted Fever. Dr. Klenner was an authority in the treatment of this rather debilitating, serious disease because his practice was right in the middle of a constant locus of infection for tick bite fever. Dr. Klenner had been taught in his training that there was no cure for it, only supportive. So when he was confronted with an obvious case—104.4° degree temperature, spots over body, coma, and positive blood test—he quickly gave 30 grams of C intravenously every six hours. The patient was given para-aminobenzoic acid orally, six grams, every two hours x3, then 4 grams every two hours for 24 hours, then 4 grams every 4 hours until his fever was gone for 24 hours. At about the sixth hour of treatment he became conscious and rational. He was sent home on the sixth day, fully recovered. The C is given around the clock and at the 500-900 mg per kg body weight level. The disease “can always be reversed.”
-Dr. Klenner reports on other research: Vitamin C inactivates the toxin of tetanus. He felt that the number of fatalities from the disease were equal to the number of those who die from the treatment. He emphasized some principles of treatment 30 to 40 years ago that many of us have forgotten: namely, do no harm, and the body has tremendous restorative powers if the doctor will supply it with the raw materials to promote recovery.
–Chronic cystitis is usually associated with alkaline urine. Germs grow more easily in this alkaline urine. Vitamin C will discourage these bacteria and cut the chance of an ascending infection which might devastate the kidneys (pyelitis). Ten grams of C per day are suggested.
-For acute alcoholism Dr. Klenner has given 1000 mg of thiamin intramuscularly every two hours until recovery. Pyridoxine, 500 mg is given every six hours. 40 grams of C intravenously will detoxify the patient.
–Arthritis: Vitamin C counteracts the damaging effects of aspirin. C is the number one precursor for collagen formation. If serum levels of C are high, synovial fluid is thinner allowing for easier joint movement. Those taking 15 to 25 grams daily will experience commensurate benefit. Prevention seems prudent. “A person who will take ten to twenty grams of ascorbic acid a day along with other nutrients might very well never develop arthritis.”
–Cancer: He cites Schlegel’s (Tulane University) use of ascorbic acid (1.5 grams a day only) in preventing bladder cancer recurrence. “This is the so called wasted Vitamin C.” He “demonstrated that in the presence of ascorbic acid, carcinogenic metabolites will not develop in the urine. They suggested that spontaneous tumor formation is the result of faulty tryptophan metabolism while urine is retained in the bladder.” Other researchers report that the depletion of mast cells from guinea pig skin was due to ascorbic acid deficiency. It suggests Vitamin C is necessary for the formation and maintenance of mast cells. Vitamin C will control myelocytic leukemia with 25-30 grams orally daily. “How long must we wait for someone to start continuous ascorbic acid drip for two to three months, giving 100 to 300 grams each day, for various malignant conditions?
–Small basal cell epithelioma: 30% Vitamin C ointment.
-His protocol for treating cancer is printed here in total. All of this is designed to kill the cancer cells by shoring up the immune system.
[Note: Back then there was less industrial pollution, no GMOs and less toxicity in general. The dietary guidelines in this diet make no sense in that they contain too much sugar and protein. A ketogenic diet is the one thing that is showing differences for cancer patients nowadays. For more info see Ketogenic diet may be key to cancer recovery.]
- Use radioactive cobalt when and where indicated.
- Give 45 grams of sodium ascorbate intravenously every twelve hours for one month. Then use 60 to 65 grams in 500 cc of normal saline or 5% dextrose in water for five days a week until a cure is obtained. It usually takes five months.
- Each bottle is to contain one gram of calcium gluconate, a cc of some B complex, plus 1,200 mg of thiamin, 300 mg of pyridoxine, and 600 mg of niacinamide.
- Oral sodium ascorbate, 5, 10, 20, grams daily. The dose depends upon the bowel tolerance.
- Vitamin A palmitate, 50,000 units, daily, orally.
- Pantothenic acid, (B5) one gram orally four times a day.
- Amino acid protein powder with all the eighteen amino acids. 60 tablets each day or, if a powder, several tablespoons daily. This supports the immune system and the enzymes. Tyrosine should be taken separately, if possible, as this one makes the others work better; 500 mg tablets—six daily.
- In addition, a high protein diet using white chicken meat, fresh fish, chicken livers, and brown-shelled eggs. Beef (but once a week) should be as lean as possible: lean stew beef or sirloin tip are the best but have the butcher grind it three times. Hamburgers? Only once a week. No sugar and no starches. Fruit and fruit juices are permitted. Almonds are excellent.
- 30 to 40 apricot almonds should be chewed every day in divided doses until a continuous bitter almond taste develops. At this point the patient cuts the dose in half. “This will form cyanide by way of the stomach acid. Cyanide will kill cancer cells. Vitamin C will protect one against the lethal effects of cyanide. It is the antidote. 500 mg tablets of vitamin B17 are available. One after each meal and at bed time.” (Not everyone would agree with this part of the therapy. Cancer victims are still getting amygdalin B17, as injections from Mexico, but there is some doubt as to its efficacy. LHS)
- Vitamin E, d-alpha tocopheryl acetate, 400 International unit size, 3,200 units daily. Don’t take iron with it.
- One pint of grape juice daily.
- B complex tablets with 100 mg of each of the B’s and 100 mcg of B12. Six to eight tablets daily. Theragran-M or a similar capsule with all the minerals to replace what is being pulled out by the C.
- Maintain the hemoglobin at 13 grams.
- Keep a good attitude.
He reported a case of a man with lymph glands all over his body. He got the above treatment and although the glands increased in size for a while, his liver and spleen were back to normal size in four months. Dr. Klenner noticed a ‘parachute-like’ substance in the urine. Microscopic examination revealed they were clumps of cancer cells.
Another case was that of a woman who had an adenocarcinoma of two years duration. She had had chemotherapy, two surgeries and extensive radiation over her chest, especially the neck area where the cancerous glands were. The cancer had spread to her lungs, her abdomen and six glands in her neck. Dr. Klenner gave her the above protocol. In three months the lesion in her lung had cleared and gone were the glands in her neck. After six months of intravenous Vitamin C and the B complex, the abdominal masses had disappeared, but she could not swallow food. The radiation had scarred her esophagus beyond dilatation and she refused more surgery. The cancer was gone; she died from starvation due to the radiation.
Dr Klenner summarized this paper with this: “The results suggest that larger daily amounts could be given in a hospital with faster results. I would suggest at least 100 grams in 1000 cc of fluid and given every twelve to 24 hours. The vitamins and the calcium gluconate also must be given.” He thought interferon could be assayed while the patient is in the hospital. “How long will it take for the general population to challenge the drug cartel?”
-There is a relationship of Vitamin C and cholesterol. Scorbutic guinea pigs have high cholesterol levels. Way back in 1947 high intravenous doses of Vitamin C were found effective in lowering cholesterol levels. Cholesterol levels in the blood of subjects vary with the amount of C used. In one patient the cholesterol was lowered 42 mg percent in six weeks when his oral intake of Vitamin C was increased from 10 grams a day to 20 grams a day. Extra C seems to be critical especially in those with a family tendency. [And as long as there is no excess iron in the body, cholesterol itself will be less likely to be toxic]
–Cavities: A gram of Vitamin C every day for each year of life (five grams a day for the five year old) will prevent cavities. Ten grams a day from age ten years for a lifetime should maintain that advantage.
–Disc, ruptured intervertebral: will be prevented with the ten-grams-a-day dose. Adequate amounts seem necessary for disc metabolism and maintenance.
-Corneal ulcers: healed with but 1.5 grams of C daily. The pain of a corneal burn was relieved immediately with twelve grams of C intravenously. The cornea was normal in 24 hours.
-He reported the story of a seven year old diabetic, who developed measles, and his insulin requirements went from 5 units to more than 90 units a day, but with one gram of Vitamin C every four hours his infection and elevated blood sugar came under control. In these diabetic cases, the Vitamin C can be cut back to reasonable levels after the infection is under control. Large prolonged doses of “Vitamin C might prove undesirable due to its dehydrating and diuretic powers.”
-As a matter of fact Dr. Klenner had been studying the effects of ten grams of C per day orally in patients with diabetes mellitus; 60% were able to control the condition with diet and C. The other 40% were able to reduce the insulin dose. Wounds healed more readily.
–Glaucoma: patients use 35 grams of C (100 mg/kg after meals and bedtime) in divided doses during the 24 hours and this osmotic dehydration of the eyeball was safe and effective. “The size of the dose does make a difference—a real difference.”
–Schizophrenia: Dr. Klenner reminds us of Hoffer and Osmond’s work with niacin and Vitamin C back in the early 1950’s. Six to 8 grams of C a day made the niacin work. One schizophrenic took one gram every hour for 48 hours and was completely recovered for six months with no further treatment. These megadoses halved the suicide rate. It has been demonstrated that schizophrenics burn up C ten times faster than the normal population.
–Burns: can be treated with Vitamin C. “30-100 grams of Vitamin C is the proper amount to employ.” (500 mg per kg of body weight diluted to at least 18 cc per gram of C using 5% dextrose or saline in water or Ringer’s solution, repeated every eight hours for several days, then at twelve hour intervals. Calcium gluconate is added.) “Vitamin C is given until healing takes place.” It takes seven to thirty days depending upon the degree of the burn. It may prevent the need for grafting as it keeps the tissues oxygenated thus preventing the blood from sludging. [Kniseley] On the fourth to fifth day the malodorous burn eschars will fall off leaving normal tissue. Vitamin C also eliminates pain; opiates are less necessary. (It stimulates endorphin production in the brain.) Three percent ascorbic acid solution is used as a spray every two to four hours for five days. Pseudomonas: (a nasty bacteria, often seen in burn patients; very resistant to antibiotics): three percent spray plus massive injections.
–Heat stroke: 500 mg per kg of body weight will reverse it.
–Sunburn: One gram taken every one to two hours during exposure will prevent sunburn; an I.V. injection will quickly relieve the pain and erythema. Even second-degree burns will be healed.
-Prickly heat, heat stroke, heat collapse can all be treated; the latter needs twelve to forty grams intravenously. Electric shock patients must be given Vitamin C immediately after the accident—including lightning victims.
-Vitamin C will control the side effects of radiation including radiation burns. “Who can say what 100 to 300 grams given intravenously daily for several months might accomplish in cancer? The potential is so great and the employment so elementary that only the illiterate will continue to deny its use.”
–Surgery: Way back in 1960 and again in 1966, Dr. Klenner delivered papers before the Tri-State Medical Society calling attention to the “scurvy levels” of C in post-operative patients. The levels began to fall six hours after surgery and by 24 hours the levels were 3/4 lower than pre-op. Tensile strength of healing wounds is lowered if the plasma drops to scurvy levels. The lower the C levels the poorer the wound heals. Even as little a dose as 500 mg of C orally “was remarkable successful in preventing shock and weakness,” following dental extraction.
-Dr. Klenner used 10 grams preoperatively intravenously and ten grams in each post-operative bottle and then ten grams orally when eating was resumed. Surgical wounds rarely separated with this method. Fractures healed faster. (Some surgeons will give ten grams of Vitamin C at the end of the operation, and the patient is awake and alert in 60 seconds. No need for the nausea and vomiting in the recovery room.)
–Heavy Metal Poisonings: Especially lead and mercury—are controlled with Vitamin C injections and oral intake. An intake of Vitamin C daily will protect animals—and by extrapolation, humans—from fatal doses of mercury. If a guinea pig needed 200 mg one day to protect it from an otherwise fatal dose of mercury, the human would need 14 grams daily. Smaller doses would be able to protect the body from smaller amounts of the toxin.
-Lead poisoning: 350 mg of Vitamin C per one kg of body weight taken intramuscularly every two to four hours; recovery in less than 72 hours.
-Dr. Klenner found that the amount of C used “in any case is the all important factor. In 28 years of research we have observed that 30 grams each day is critical in terms of response” regardless of age and weight. (Barbiturate intoxication, snake bite and viral encephalitis may require larger doses in some individuals.)
–Carbon Monoxide (CO): if 12 to 50 grams of Vitamin C is injected rapidly into the blood stream, it acts as an oxidizer and will “pull CO from hemoglobin to form carbon dioxide” which is easily exhaled. A burn victim should immediately receive a dose of 500 mg of C per kg of body weight intravenously. It will “neutralize the CO or smoke poisoning while at the same time it will prevent blood sludging which in the major factor in the development of third degree burns.” An accidental carbon monoxide poisoning was reversed in ten minutes with 12 grams of ascorbic acid in a 50 cc syringe using a twenty gauge needle. (”We employ a twenty-gauge needle when using a 50 cc syringe; a twenty-one gauge for a thirty-cc syringe, a twenty-two gauge for a twenty cc syringe and a twenty-three gauge needle for a ten cc syringe“).
-In another Tri-State Medical Journal of December, 1957, he outlined the physiology and treatment of Black Widow Spider poisoning in a case history. Some of those bitten are not affected at all because the spider was out of poison, but some can be devastated and may die, partly because of poor resistance but also due to the quantity injected. It can be confused with pancreatitis, renal colic, food poisoning, tetanus, angina, bowel obstruction, pneumonia, perforated ulcer. The abdominal wall muscles become rigid, the victims have cold sweat, their temperature and blood pressure shoot up, they vomit, have muscle twitches and spasms, cyanosis, chills, convulsions and delirium. The painful muscle spasms occur within minutes of the original bite. The cramps occur in all the large muscles of the body; the victims roll and toss and moan in agony. Until someone used calcium gluconate, there were 90 ineffective treatments. An anti-venom is on the market, but severe reactions and even death have been attributed to its use. The treatment Dr. Klenner suggests is his friend, Vitamin C, 350 mg per kg of body weight intravenously along with calcium gluconate. His three and a half year old patient had been getting worse for 24 hours with abdominal cramps which the parents assumed were due to food poisoning. She became quieter, feverish, constipated and her abdomen was exquisitely tender. She was becoming stuporous. Dr Klenner noted the red, swollen area around her naval, and two tiny spots about one eighth of an inch apart were noted in the middle: the fang marks of a Black Widow Spider. He gave one gram of calcium gluconate and 4 grams of Vitamin C intravenously. In 6 hours she was more responsive, and her temperature had dropped from 103 degrees to 101 degrees and she was given another four grams I.V. “Some ascorbic acid behaves much like calcium in the body, and also acts synergistically with it, we elected to observe its action.” The child was destined to die. “Some physicians would stand by and see their patient die rather than use ascorbic acid because in their finite minds it exists only as a vitamin.”
-Dr. Klenner was very confident about the benefits of intravenous Vitamin C to treat the poisonous effects of insects and reptiles,. He felt all emergency rooms should be adequately stocked. He used sodium ascorbate, 7.5 grams in 30 ml. The syringes are 5 to 60 cc. The needles are 20 gauge (big), one inch long to 31 gauge (I have trouble believing this) one inch long. I get “miracle like responses.”
-“Sodium ascorbate will cure any type of snake bite.” The amounts and the speed of injection are critical. Forty to 60 grams intravenously as a starter. Klenner cites the 6500 deaths a year from snake bites, but many more from insects, bees, spider, plants and some caterpillars. They produce formic acid, histamine and specific toxin albumins. Some are neurotoxins; some cause capillary damage and hemorrhage. When cells are damaged proteins are deaminized, producing histamine and other toxic products; shock may occur. These deaminizing enzymes from the damaged cells are inhibited by Vitamin C. The pH of cells changes when cells are damaged; enzymes become destructive instead of constructive. C reverses this. Vitamin C is reduced in the serum of those in shock. 350-700 mg per kg body weight is the saving intravenous dose. In children up to two grams can be given in each of several areas (a twenty kg five year old could get two grams in each of four sites. Ice before and after the injection would control the pain).
–Multiple Sclerosis & Myasthenia Gravis. Adequate oxygen is assured if the lungs and hemoglobin are normal, but also by taking 10 to 30 grams of ascorbic acid by mouth every 24 hours. Oxygen is released for tissue use when ascorbic acid becomes dehydroascorbic acid. Enzymes are necessary to make all these reactions possible. Genetic faults manifest themselves through enzymatic deficiencies. He puts Myasthenia Gravis and Multiple Sclerosis in the same therapeutic group as he found thiamin was the key to the therapy. M.G. is a genetically transmitted disease and M.S. is triggered by a virus and mimics poliomyelitis. Nerve damage in M.S. is due to microscopic hemorrhages in the nervous system. During healing, scar tissue contracts clamping off capillary flow and nutrition. This wasting results in loss of the myelin sheath protection. He felt that remyelinating these damaged nerves was every bit as hopeful as the myelination that occurs normally in infancy with nothing more spectacular than breast milk. It requires two years of treatment to repair the damage caused by one year of the disease. He cites works in the late 1930s by Stern at Columbia University who used thiamin intraspinally for the treatment of Multiple Sclerosis with astonishing results. After 30 mg of thiamin was injected into the spinal canal of paralyzed MS. victims, they had a temporary remission. Dr. Klenner felt that most cases (80%) of Multiple Sclerosis had their origin in an illness—probably a coxsackie virus—compatible with a summer “flu”. He mentioned other theories of the etiology of M.S., but was convinced that the scar tissue that forms around the nerves and produces the symptoms “is the end result of microscopic hemorrhages following virus invasion.”
-Dr. Klenner reports on a few minor complications. Some diarrhea might have been due to sodium bisulfite. Induration after intramuscular injections was found to be due to the Vitamin C not being injected deeply enough into the muscle. (One had to be drained—a sterile abscess.) If the concentration was one gram to 5 cc it caused a vein spasm up the arm from the injection site in three cases. A thrombosis of the vein occurred in but one case. A minor face rash developed in a few that cleared after the C was stopped. Calcium seemed to enhance the effects of the C when both were give simultaneously. But a gram of just the calcium given intravenously can slow the heart rate to a dangerous degree.
-Oxalic acid precipitates out of solution only from a neutral or alkaline solution—pH 7 to pH 10. Urine pH in those consuming ten grams of Vitamin C daily is about 6. Even in diabetics who take this large amount of C (10 grams), the urinary oxalate excretion remains relatively unchanged. “Vitamin C is an excellent diuretic. No urinary stasis; no urine concentration. The ascorbic acid/kidney stone story is a myth.” One more bon mot: “Methylene will dissolve calcium oxalate stones, if the patient is given 65 mg orally two to three times a day,” he learned from Medical World News (Smith, M.J.V., M.D.: Dec. 4, 1970). (90% of all stones are calcium stones. Calcium is soluble in acid media. Vitamin C acidifies the urine. Acid urine discourages the growth of bacteria. Although uric acid stones are theoretically possible with high doses of C and a low urinary pH, none have been reported.)
-He reiterates the safety of large doses of C. He states that plasma doses of greater than twenty times normal produce no ill effects. Diarrhea is the most common side effect of large doses. Some notice thickening of subcutaneous tissue is the C is not injected deeply enough into, the muscle. (That induration will eventually resolve.) Some will complain of venous irritation and spasm if the intravenous Vitamin C is too concentrated or too rapidly injected. (C mixed with calcium will reduce this irritation.) A rare thrombosis may occur if the concentration of the C is greater than 500 mg per cc. Some will faint if the injection is given too rapidly. (It is best to have the patient lie flat.) Large doses by mouth may cause a genital or anal rash and itch. He also showed how safe large doses of C were. He gave 200 patients 500 to 1000 mg of C every four to six hours for five to ten days. No laboratory abnormalities were found in blood or urine and no symptoms were noted except one percent who developed vomiting; he assumed from a hypersensitive stomach. And these patients had no virus infection to “assist in destroying the vitamin.”
Current IV Vitamin C Guidelines
Nowadays baseline blood tests include screening for red blood cell glucose-6-phospahte dehydrogenase deficiency. Those with G6PD, an extremely rare condition, can have problems of hemolysis when vitamin C at large doses are first infused.
In case of iron overload, vitamin C is also discouraged as it will increase iron’s absorption, often carrying its toxic effect into the heart. Due to iron overload’s pro-cancer and pro-disease effects, many people will find themselves not able to benefit from vitamin C. These people will only recover their health and energy with iron chelation therapies such as EDTA and bloodletting. Yes, donating blood can be very good for your health!
There are numerous case histories where vitamin C’s anti-cancer properties have been reported. You’ll find resources on where these therapies are performed at Orthomolecular.org.
Usually a protocol will look like this:
Week 1: 1 x 15 g infusion per day, 2-3 per week.Week 2: 1 x 30 g infusion per day, 2-3 per week.
Week 3: 1 x 65 g infusion per day, 2-3 per week.
The dose is then adjusted to achieve blood concentrations of 400mg/dL, 2-3 infusions per week. Sodium ascorbate is the one usually used for IV vitamin C infusion, as it is more friendly.
Lots of folks just do their own liposomal vitamin C and voilà.
Interesting article from the Riordan Clinic
Their iv protocol looks like this:
the article has tons of other information and some clinical data.
Their iv protocol looks like this:
THE RIORDAN IVC PROTOCOL
Inclusion Criteria and Candidates
- Candidates include those who have failed standard treatment regimens; those seeking to improve the effectiveness of their standard cancer therapy; those seeking to decrease the severity and carcinogenicity of side effects from standard cancer therapy; those attempting to prolong their remission with health-enhancing strategies; those declining standard treatment, yet wishing to pursue primary, alternative treatment.
- Patient (guardian or legally recognized care-giver) must sign a consent-to-treat or release form for the IVC treatment. Patient should have no significant psychiatric disorder, end-stage CHF, or other uncontrolled co-morbid conditions.
- Obtain baseline and screening laboratory:
- Serum chemistry profile with electrolytes
- Complete blood count (CBC) with differential
- Red blood cell G6PD (must be normal)
- Complete urinalysis
- In order to properly assess the patient’s response to IVC therapy, obtain complete patient record information prior to beginning IVC therapy:
- Tumor type and staging, including operative reports, pathology reports, special procedure reports, and other staging information. (Re-staging may be necessary if relapse and symptom progression has occurred since diagnosis.)
- Appropriate tumor markers, CT, MRI, PET scans, bone scans, and x-ray imaging.
- Prior cancer treatments, the patient’s response to each treatment type, including side effects.
- The patient’s functional status with an ECOG Performance Score.
- Patient weight.
Precautions and Side Effects
In the Riordan Clinic’s experience giving over 40,000 onsite IVC treatments, the side-effects of high-dose IVC are rare. However, there are precautions and potential side-effects to consider.
- The danger of diabetics on insulin incorrectly interpreting their glucometer finger stick has been found. It is important to notice to health care workers using this protocol for the treatment of cancer in patients who are also diabetic: high dose intravenous vitamin C (IVC) at levels 15 grams and higher will cause a false positive on finger-stick blood glucose strips (electrochemical method) read on various glucometers (Jackson & Hunninghake, 2006). Depending on the dose, the false positive glucose and occasionally “positive ketone” readings may last for eight hours after the infusion. Blood taken from a vein and run in a laboratory using the hexokinase serum glucose method is not affected! The electrochemical strip cannot distinguish between ascorbic acid and glucose at high levels. Oral vitamin C does not have this effect. Please alert any diabetic patients of this potential complication! Diabetics wishing to know their blood sugar must have blood drawn from a vein and run in the laboratory using the hexokinase glucose determination method.
- Tumor necrosis or tumor lysis syndrome has been reported in one patient after high-dose IVC (Campbell & Jack, 1979). For this reason, the protocol always begins with a small 15 gram dose.
- Acute oxalate nephropathy (kidney stones) was reported in one patient with renal insufficiency who received a 60 gram IVC. Adequate renal function, hydration, and urine voiding capacity must be documented prior to starting high-dose IVC therapy. In our experience, however, the incidence of calcium oxalate stones during or following IVC is negligible (Riordan, et al., 2005).
- Hemolysis has been reported in patients with G6PD deficiency when given high-dose IVC (Campbell, et al., 1975). The G6PD level should be assessed before beginning IVC. (At the Riordan Clinic, G6PD readings have yielded five cases of abnormally low levels. Subsequent IVC at 25 grams or less showed no hemolysis or adverse effects.)
- IV site irritation may occur at the infusion site when given in a vein and not a port. This can be caused by an infusion rate exceeding 1.0 gram/minute. The protocol suggests adding magnesium to reduce the incidence of vein irritation and spasm.
- Due to the chelating effect of IVC, some patients may complain of shakiness due to low calcium or magnesium. An additional 1.0 mL of MgCl added to the IVC solution will usually resolve this. If severe, it can be treated with an IV push of 10 mL’s of calcium gluconate, 1.0 mL per minute.
- Eating before the IVC infusion is recommended to help reduce blood sugar fluctuations.
- Given the amount of fluid used as a vehicle for the IVC, any condition that could be adversely affected by fluid or sodium overload (the IV ascorbate is buffered with sodium hydroxide and bicarbonate) is a relative contraindication; i.e. congestive heart failure, ascites, edema, etc.
- There have been some reports of iron overload with vitamin C therapy. We have treated one patient with hemochromatosis with high-dose IVC with no adverse effects or significant changes in the iron status.
- As with any I.V. infusion, infiltration at the site is possible. This is usually not a problem with ports. Our nursing staff has found that using #23 Butterfly needles with a shallow insertion is very reliable with rare infiltrations (depending upon the status of the patient’s veins!)
- IVC should only be given by slow intravenous drip at a rate of 0.5 grams per minute. (Rates up to 1.0 gram/minute are generally tolerable, but close observation is warranted. Patients can develop nausea, shakes, and chills.)
- It should never be given as an IV push, as the osmolality at high doses may cause sclerosing of peripheral veins, nor should it be given intramuscularly or subcutaneously. The accompanying table lists the calculated osmolality of various amounts of fluid volume. Our experience has found that an osmolality of less than 1200 mOsm/kg H2O is tolerated by most patients. A low infusion rate (0.5 grams IVC per minute) also reduces the tonicity, although up to 1.0 grams per minute can be used in order to achieve higher post IVC saturation levels. (Pre and post serum osmolality measurements are advisable at this dose.)
- We presently use a sodium ascorbate solution, MEGA-C-PLUS®, 500 mg/mL, pH range 5.5-7.0 from Merit Pharmaceuticals, Los Angeles, CA, 90065.
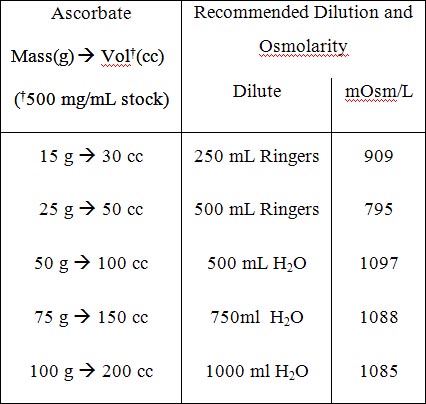
Table 1: Recommended Dilution and Osmolarity
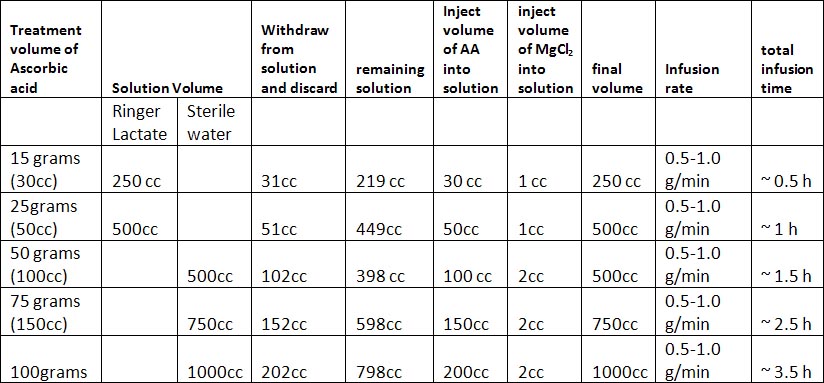
Table 2: Treatment Volume of Ascorbic Acid
Administration of IVC
Having taken all precautions listed above and having obtained informed consent from the patient, the administering physician begins with a series of three consecutive IVC infusions at the 15, 25, and 50 gram dosages followed by post IVC plasma vitamin C levels in order to determine the oxidative burden for that patient so that subsequent IVCs can be optimally dosed.
The initial three infusions are monitored with post IVC infusion plasma vitamin C levels. As noted above (Scientific Rational), research and experience has shown that a therapeutic goal of reaching a peak-plasma concentration of ~20 mM (350- 400 mg/dL) is most efficacious. (No increased toxicity for post IVC plasma vitamin C levels up to 780 mg/dL has been observed.) The first post IVC plasma level following the 15 gram IVC has been shown to be clinically instructive: levels below 100 mg/dL correlate with higher levels of existent oxidative stress, presumably from higher tumor burden, chemo/radiation damage, hidden infection, or other oxidative insult, such as smoking.
Following the first three IVCs, the patient can be scheduled to continue either a 25 or 50 gram IVC dose (doctor’s discretion) twice a week until the post IVC plasma level results are available from the lab. If the initial 50 gram post IVC level did not reach the therapeutic range of 350 – 400 mg/dL, another post IVC vitamin C level should be obtained after the next scheduled 50 gram IVC. If the therapeutic range is achieved, the patient is continued on a 50 gram twice a week IVC schedule with monthly post IVC determinations to assure continued efficacy. If the therapeutic range is still not achieved, the IVC dosage is increased to 75 grams of vitamin C per infusion for four infusions, at which time a subsequent post IVC plasma level is obtained. If the patient remains in a sub-therapeutic range, the IVC dosage is increased to the 100 gram level.
If after four infusions the post IVC dosage remains sub-therapeutic, the patient may have an occult infection, may be secretly smoking, or may have tumor progression. While these possibilities are being addressed, the clinician can elect to increase the 100 gram IVC frequency to three times per week. Higher infusion doses beyond 100 grams are not recommended without serum osmolality testing before and after infusions in order to properly adjust the infusion rate to maintain a near physiologic osmolality range.
If higher dosages are not tolerated, or there is tumor progression in spite of achieving the therapeutic range, lower dosages can still augment the biological benefits of IVC, including enhanced immune response, reduction in pain, increased appetite, and a greater sense of well-being.
Very small patients, such as children, and very large obese patients need special dosing. Small patients < 110 lbs. with small tumor burdens and without infection may only require 25 gram vitamin C infusions 2x/week to maintain therapeutic range. Large patients > 220 lbs. or patients with large tumor burdens or infection are more likely to require 100 grams IVC infusions 3x/week. Post IVC plasma levels serve as an excellent clinical guide to this special dosing.
In our experience, the majority of cancer patients require 50 gram IVC infusions 2-3x/week to maintain therapeutic IVC plasma levels. All patients reaching therapeutic range should still be monitored monthly with post IVC plasma levels to ensure that these levels are maintained long term. We advise patients to orally supplement with at least 4 grams of vitamin C daily, especially on the days when no infusions are given, to help prevent a possible vitamin C “rebound effect.” Oral alpha lipoic acid is also recommended on a case by case basis.
the article has tons of other information and some clinical data.
Excerpt from The Dr. Ewan Cameron Vitamin C Treatment Protocol for Cancer
[...]
INTRAVENOUS VITAMIN C
Vitamin C intravenously can be given by intermittent injection, but this is not recommended, particularly if the intervals between injections extend to several days. Because of the rebound effect, such administration would produce a sawtooth plasma ascorbate profile with abnormally low levels in the troughs just prior to the next injection. We recommend continuous administration via slow drip infusion.
It is recommended that the patient be hospitalized for initial evaluation and commencing the intravenous regimen. Intravenous vitamin C can cause troublesome chemical phlebitis if injected directly into a superficial vein. For this reason it is recommended that infusion be given via a C.V.P. (Central Venous Pressure, or similar) line, with routine A-P portable chest X-ray taken after placement to ensure that the catheter tip is correctly positioned in the Superior Vena Cava. Alternately a "Hep-Lock" (or similar) cannula may be used in a forearm vein with appropriate precautions against clotting.
(Additional information on intravenous vitamin C administration is found in A Physician's Handbook of Orthomolecular Medicine, Roger J. Williams, editor; at the website of Robert Cathcart, MD (http://www.orthomed.com); in Dr. Cathcart’s paper entitled Preparation of Sodium Ascorbate for IV and IM Use posted at DoctorYourself.com - Preparing Vitamin C for I.V. administration ; and in Clinical Guide to the Use of Vitamin C, by Lendon Smith, MD. The full text of Dr. Smith’s book is posted at http://www.seanet.com/~alexs/ascorbate/198x/smith-lh-clinical_guide_1988.htm . These sources discuss details including needle gauges and buffers, among other topics.)
The recommended "carrier solution" is Ringer's Lactate Solution, readily available in liter packs or flasks, and infused at the steady rate of 2 liters (two packs) every 24 hours. Isotonic Dextrose should never be used as the carrier solution. Vitamin C for parenteral use comes in sterile ampules of sodium ascorbate preferably without preservative. Standard ampules contain 0.5g (500 milligrams), or as "multiuse" 50 ml ampules containing 25 grams. The ampules should be added to the infusion packs under full sterile conditions in the Hospital Pharmacy or Infusion Fluids Department.
In patients not previously exposed to high levels of ascorbate, a gradual "wind-up" dose regimen is recommended, along the following lines:
Day One to the first flask add 0.5g sodium ascorbate
to the second 1.0g sodium ascorbate
to the third 1.5g sodium ascorbate
to the fourth 2.0g sodium ascorbate
Day Two to the fifth flask add 2.5g sodium ascorbate
(continuing at that level infuses 10g sodium ascorbate per day)
Much higher doses can be and have been infused with perfect safety, the limiting factor being sodium overload with water retention, and not the ascorbate ion itself. The wind-up dosage schedule is not necessary in patients receiving "booster" repeat courses.
PRECAUTIONS: Standard continuous infusion procedure must be followed. It is not necessary to monitor serum electrolyte levels except in patients with gross cardiac or renal impairment.
SIDE-EFFECTS There are two recognized side-effects, one very common and relatively harmless, the other very rare and highly dangerous. The common side-effect is transient fluid retention due to sodium overload resulting in some ankle edema in the ambulant and sacral pad edema in those confined to bed. Inpatients with cardiac impairment dangerous pulmonary edema may develop and require intravenous frusemide for its control.
The rare side-effect, seen only in patients with highly anaplastic very rapidly growing tumors and a heavy tumor load, is the sudden precipitation of widespread tumor necrosis. Clinically this is heralded by sudden pain in all tumor deposits, rapid swelling of known tumors, tumor hemorrhage, both internal and external, hyperpyrexia, severe hypotension, tachycardia and azotemia. This very rare complication can be fatal and must be vigorously treated. If suspected, the ascorbate infusion should be immediately stopped, and the patient treated as for septicemic shock. The patient may require transfer to the Intensive Care Unit for close monitoring and support by oxygen, plasma or blood, and intravenous steroids. If resuscitation is successful, it will be found that any residual tumor has shrunk considerably or even disappeared. Although highly dangerous, this reaction might also be termed the best possible response to ascorbate treatment of wide-spread cancer.
ORAL VITAMIN C
On the day planned to terminate intravenous ascorbate, the patient should be commenced on oral ascorbate at the same daily intake. The medication should be taken every six hours (four times a day), and once commenced should never be abruptly discontinued because of the rebound effect. The dose varies between individuals in the 10 to 30g a day range. The aim should be to maintain plasma ascorbate levels of at least 3mg/dl for effective therapy. Leukocyte ascorbate concentration, a technically more difficult estimation to perform, is of much less value in predicting response to treatment.
RESPONSE TO ASCORBATE TREATMENT
As with any other form of cancer treatment, therapeutic response will vary between individual patients, with paradoxically the best responses seen with individuals with far advanced disease. Therapeutic responses may be listed as follows:
1. No response detectable (a very few)
2. Some retardation of progressive tumor growth (very many)
3. Stasis or standstill effect (considerable number)
4. Tumor regression (a few)
5. Tumor necrosis (very rare)
A typical response to ascorbate can be described as follows:
An improvement in well-being, vigor and Karnovsky performance status will be apparent in 5 to 7 days. Originally thought to be a purely subjective response, it is now realized to be objective and due to restoration of endogenous carnitine biosynthesis, carnitine being responsible for transporting triglycerides across the mitochondrial membrane where they are burned for muscle energy.
If painful skeletal metastases are present, relief of bone pain will occur in about 5 to 7 days, enabling opiates to be withdrawn without withdrawal symptoms. Skeletal or widespread visceral metastases are associated with increased urinary hydroxyproline (UHP) excretion reflecting collagen breakdown. Within 5 days of commencing ascorbate therapy, a sharp and sustained fall in UHP excretion will be noted.
Response to treatment will also be reflected in a drop in the sedimentation rate and fall in the titer of any serum tumor protein markers (CEA etc.) if present.
Radiological signs of good response include the slow conversion of osteolytic skeletal metastases to dense osteosclerotic lesions over a period of months. In favorable cases, resorption of malignant pleural effusions and reduction in size of pulmonary metastases have been observed.
CONTINUATION OF TREATMENT
Oral ascorbate should be continued indefinitely and the patient carefully monitored at least every month. The usual course of events is that the patient instead of slowly declining will enter a plateau of comparative well-being that may continue for many months or even years, and then enter an abrupt downhill phase with explosive metastases. At the first suspicion of this change, a "booster" course of intravenous ascorbate is recommended, even though individual responses can never be predicted. Over a period of three years, one patient with widespread leiomyosarcoma had six such booster courses with clear benefit from each one except the last. Many other patients have shown no benefit from even the first booster course, but it is always worth trying.
[...]
nature
Dagobah Resident
Hi Ant22 !I just bought some sodium ascorbate and I will be "investigating it" this weekend. I'll report if I notice any results worth mentioning.
You can do your own sodium ascorbate, to save money. Here is the tip for ascorbate enema:
- Vitamin C quickly oxidizes in water, so you might prepare it at the last moment, just before use.
- Mix in a bowl : pure powder of Vitamin C (maximum 20 g for this volume) and sodium bicarbonate (half the dose of Vitamin C). Personnally, I used only 3 to 5 g per enema the first time I used this method as it was new for me. It was an enema each 2 or 3 hours, so I got roughly 30g a day .
Add warm water and mix well. L-ascorbic acid + sodium bicarbonate = sodium L-ascorbate (Vitamin C neutral pH) + CO2 (gas, you will see bubbles in the bowl).
- Do your enema as in cofee enemas.
- Wait 8 to 10 minutes for your mucous membranes to absorb Vitamin C. After 8-10 minutes, you'll feel the need to go to toilet: flush the remaining liquid into the toilet bowl and do rinse the pear and wash the cannula with soap.
I buy my vit c powder on this french site, as it is organic and without additives; they ship in europe for free. Hope this helps.
Wow, check this out. I've also been looking for articles on IV vitamin C treatment for babies and children, and I found this paper published in 2016, so it's pretty recent. In this case, they used the Riordan Protocol that nicklebleu mentions above. "High-Dose Intravenous Vitamin C Treatment of a Child with Neurofibromatosis Type 1 and Optic Pathway Glioma: A Case Report"
The patient (poor little guy has an optic pathway tumor):
Some interesting bits:
Notice that the size of the tumor increased after (IMO, the useless) chemotherapy, and decreased greatly in size after IVC treatment!
It seems that IVC treatment should be given weekly for a prolonged period (years) for the cancer/tumor to be 'dissolved' (hopefully), at least in this case. See a short description of the protocol here:
He hasn't stopped and continues to receive treatment, at the time the paper was written and published:
In the Discussion section, there is this information, which is interesting for me personally as I have corneal damage/scarring (and to those who may be suffering from cerebral tissue degeneration):
See what they write about vitamin D:
This is the source for the protocol they mention: 26. Riordan H, Riordan N, Casciari J, et al. The Riordan Intravenous Vitamin C (IVC) Protocol. In: Saul AW, editor. Book [The Orthomolecular Treatment of Chronic Disease,] Basic Health publication. 2014. pp. 750–66. Appendix 3:
More info on the Riordan Protocol can be found here: http://www.doctoryourself.com/RiordanIVC.pdf
All in all, another promising case.
The patient (poor little guy has an optic pathway tumor):
We describe the case of a 5-year-old child who was diagnosed with NF1 and optic pathway tumor onset at the age of 14 months. Because of the tumor progression, chemotherapy with carboplatin and vincristine was prescribed at this early age and continued for one year. As the progression of disease continued after chemotherapy, the child, at the age of 2.8 years, was started on high-dose intravenous vitamin C (IVC) treatment (7–15 grams per week) for 30 months. After 30 months, the results of IVC treatments demonstrated reduction and stabilization of the tumors in the optic chiasm, hypothalamus, and left optic nerve according to radiographic imaging. The right-sided optic nerve mass seen before IVC treatment disappeared by the end of the treatment.
Some interesting bits:
Changes in the hypothalamic component before and during IVC treatment are shown in Figure 3 and demonstrate the reduction in the size of tumor during IVC treatments. According to the data in Figure 3, the size of hypothalamic/optic chiasm tumor had increased about two times at the end of chemotherapy, remained the same size at the beginning of the IVC treatment, and decreased about five times during two years of IVC treatment .
Notice that the size of the tumor increased after (IMO, the useless) chemotherapy, and decreased greatly in size after IVC treatment!
It seems that IVC treatment should be given weekly for a prolonged period (years) for the cancer/tumor to be 'dissolved' (hopefully), at least in this case. See a short description of the protocol here:
The patient received IVC injections once per week (7 g at the first visit, 10 g the next 4 weeks, and after that 15 g per week, for a total of 100 treatments).
He hasn't stopped and continues to receive treatment, at the time the paper was written and published:
The patient still comes to the clinic weekly and continues high-dose IVC treatment. The patient is monitored by our doctors, and there have been no complications caused by the treatment.
In the Discussion section, there is this information, which is interesting for me personally as I have corneal damage/scarring (and to those who may be suffering from cerebral tissue degeneration):
Ascorbic acid is essential for the formation of collagenase, a basic substance of connective tissue, which may be related to corneal wound healing and prevention of cerebral tissue degeneration.
See what they write about vitamin D:
In addition to the IVC treatment, supplementation with vitamin D may have a positive effect on the patient’s condition. Vitamin D receptors have important effects not only on physiological processes related to calcium metabolism, but also on cell growth and differentiation. There is in vitro evidence that vitamin D metabolites might be useful agents in the differentiation therapy of human malignant gliomas [38,39]. The major biologically active metabolite of vitamin D has shown a cytotoxic effect on rat and human glioma cells [40].
This is the source for the protocol they mention: 26. Riordan H, Riordan N, Casciari J, et al. The Riordan Intravenous Vitamin C (IVC) Protocol. In: Saul AW, editor. Book [The Orthomolecular Treatment of Chronic Disease,] Basic Health publication. 2014. pp. 750–66. Appendix 3:
More info on the Riordan Protocol can be found here: http://www.doctoryourself.com/RiordanIVC.pdf
All in all, another promising case.
This site summarises three cases of IV Vitamin C administration with dosages used in each case: Intravenously administered vitamin C as cancer therapy: three cases
Abstract
Early clinical studies showed that high-dose vitamin C, given by intravenous and oral routes, may improve symptoms and prolong life in patients with terminal cancer. Double-blind placebo-controlled studies of oral vitamin C therapy showed no benefit. Recent evidence shows that oral administration of the maximum tolerated dose of vitamin C (18 g/d) produces peak plasma concentrations of only 220 μmol/L, whereas intravenous administration of the same dose produces plasma concentrations about 25-fold higher. Larger doses (50–100 g) given intravenously may result in plasma concentrations of about 14 000 μmol/L. At concentrations above 1000 μmol/L, vitamin C is toxic to some cancer cells but not to normal cells in vitro. We found 3 well-documented cases of advanced cancers, confirmed by histopathologic review, where patients had unexpectedly long survival times after receiving high-dose intravenous vitamin C therapy. We examined clinical details of each case in accordance with National Cancer Institute (NCI) Best Case Series guidelines. Tumour pathology was verified by pathologists at the NCI who were unaware of diagnosis or treatment. In light of recent clinical pharmacokinetic findings and in vitro evidence of anti-tumour mechanisms, these case reports indicate that the role of high-dose intravenous vitamin C therapy in cancer treatment should be reassessed.
Thirty years ago Cameron, Campbell and Pauling reported beneficial effects of high-dose vitamin C (ascorbic acid) therapy for patients with terminal cancer.1–4 Subsequent double-blind, randomized clinical trials at the Mayo Clinic failed to show any benefit,5,6 and the role of vitamin C in cancer treatment was discarded by mainstream oncologists.7,8 Vitamin C continues, however, to be used as an alternative cancer therapy.9,10
A key distinction between conventional, science-based medicine and alternative therapy is the presence or absence of scientific plausibility.11 In conventional medicine, the efficacy of treatment is proven by properly conducted clinical trials. Many treatments are still used if there is moderately good, albeit inconclusive evidence of efficacy (“clinical plausibility”), especially when treatment rationale agrees with biologic facts (conferring “biological plausibility”).11 Vitamin C is an alternative cancer therapy because the results obtained in original studies that suggested clinical benefit were not confirmed by controlled clinical trials, and the notion that high-dose vitamin C was selectively toxic to cancer cells was biologically implausible.
New information is available pertaining to biological plausibility. Although similar doses of vitamin C were used in the Cameron–Pauling and Mayo Clinic studies, the Cameron–Pauling studies combined intravenous and oral administration whereas the Mayo Clinic studies used only oral administration.1,2,12–14Recent pharmacokinetics modeling15 indicates that with oral administration, even very large and frequent doses of vitamin C will increase plasma concentrations only modestly, from 70 μmol/L to a maximum of 220 μmol/L, whereas intravenous administration raises plasma concentrations as high as 14 000 μmol/L. Concentrations of 1000–5000 μmol/L are selectively cytotoxic to tumour cells in vitro,16–20 and emerging evidence indicates that ascorbic acid at concentrations achieved only by the intravenous route may function as a pro-drug for hydrogen peroxide delivery to tissues.20 The in vitro biologic evidence and clinical pharmacokinetics data confer biological plausibility to the notion that vitamin C could affect cancer biology and may explain in part the negative results of the Mayo Clinic trials.13,15,21,22 Thus, sufficient evidence has accumulated, not to use vitamin C as cancer treatment, but to further explore the therapeutic concept. One way to increase the clinical plausibility of alternative cancer therapies is rigorous, well-documented case reporting, as laid out in the US National Cancer Institute (NCI) Best Case Series guidelines (http://www3.cancer.gov/occam/bestcase.html).23,24 Such case series might identify alternative therapies that merit further investigation.23,24
Case reports of apparent responses by malignant disease to intravenous vitamin C therapy have appeared,25–30 including those of 2 of the 3 patients presented below.25,26 However, they were reported without sufficient detail or with incomplete follow-up for evaluation and without conforming to NCI Best Case Series guidelines. They also lacked objective pathologic confirmation, which is a pillar of NCI guidelines. In this article, we use NCI Best Case Series guidelines to report 3 cases of patients with usually progressive malignant disease who received intravenous vitamin C therapy as their only significant cancer therapy and whose clinical courses were unusually favourable. Original diagnostic material obtained before treatment with vitamin C was reviewed by pathologists at the National Institutes of Health (NIH) who were unaware of the diagnoses and treatments.
Patient 1
This case was previously reported but without long-term follow-up, without detail, and with no independent pathologic confirmation.25,26 A 51-year-old woman was found in August 1995 to have a tumour involving her left kidney. At nephrectomy in September 1995 this was shown to be a renal cell carcinoma 9 cm in diameter with thrombus extending into the renal vein. Chest radiography results were normal, and there was no evidence of metastatic disease on CT scan of the chest and abdomen. In March 1996 a CT scan of the chest indicated several new, small, rounded and well-defined soft tissue masses no larger than 5 mm in diameter; they were judged consistent with metastatic cancer. By November 1996 chest radiography revealed multiple cannonball lesions (Fig. 1).
The patient declined conventional cancer treatment and instead chose to receive high-dose vitamin C administered intravenously at a dosage of 65 g twice per week starting in October 1996 and continuing for 10 months. She also used other alternative therapies: thymus protein extract, N-acetylcysteine, niacinamide and whole thyroid extract (Table 1). In June 1997 chest radiography results were normal except for one remaining abnormality in the left lung field, possibly a pulmonary scar (Fig. 2).
In October 2001 a new mass 3.5 cm in diameter in the anterior right lung was detected on radiography. A transthoracic biopsy revealed small-cell carcinoma of the lung. The patient opted for intravenous vitamin C injections. The lung mass remained constant in size in radiograpy taken in May and August 2002 but had increased to 4 cm in views taken in October 2002. In early November hyponatremia developed. Two weeks later the patient was admitted to hospital with abdominal distension and constipation. Barium studies revealed slow transit but no intestinal obstruction. Results of a CT scan of the abdomen were normal. She died shortly afterward, and no autopsy was performed. Histopathologic review of the primary renal tumour at the NIH confirmed the diagnosis of clear-cell renal carcinoma, type, nuclear grade III/IV, with the largest diameter measuring 6.5 cm. The tumour involved the renal vein and hilar perinephric fat. Pathologic review of the lung tumour biopsy specimen of October 2001 was not conducted at the NIH. Local pathologists diagnosed this specimen as indicating small-cell lung cancer and not recurrent metastatic renal cell carcinoma.
This case describes the regression of pulmonary metastatic renal cancer in a patient receiving high-dose intravenous vitamin C therapy. According to the NCI Best Case Series guidelines, the credibility of this case would be increased by biopsy proof that the multiple slowly growing bilateral cannonball lung nodules in this patient with known renal cell carcinoma were actually malignant. However, in this case, the clinical characteristics and evolution of the pulmonary lesions, in the absence of bacterial infection or other systemic disease, make any other diagnosis unlikely. The clinician attending the patient deemed a confirmatory biopsy to be unnecessary and inappropriate in this setting. A plausible alternative explanation to the conclusion that this patient's metastatic renal cell cancer responded to intravenous vitamin C therapy is that the tumours spontaneously regressed. Spontaneous regression has been reported in renal cell cancer, but it is rare, occurring in fewer than 1% of cases and typically after nephrectomy, radiation to the primary tumour or primary tumour embolization.31,32 Here, metastatic disease appeared several months afternephrectomy, rather than regressing in response to it. As well, the primary cancer was nuclear grade III/IV and involved the renal vein, factors associated with a highly unfavourable prognosis.31
Of note, more than 4 years after stopping intravenous vitamin C therapy and with the renal cell cancer in complete remission, primary small-cell lung cancer was diagnosed in this patient, who was a long-standing cigarette smoker. The second cancer did not respond to high-dose vitamin C therapy. From the clinical history it appears the tumour remained a constant size for many months and likely slowly progressed until her death about a year after diagnosis despite the resumption of intravenous vitamin C therapy.
Patient 2
A 49-year-old man presented to his physician in 1996 with hematuria and was found at cystoscopy to have a primary bladder tumour with multiple satellite tumours extending 2–3 cm around it. Transurethral resection of the primary tumour and its surrounding tumour satellites was carried out until apparently normal muscle was reached and the tumour base was fulgurated. The patient declined systemic or intravesical chemotherapy or radiotherapy and instead chose intravenous vitamin C treatment. He received 30 g of vitamin C twice per week for 3 months, followed by 30 g once every 1–2 months for 4 years, interspersed with periods of 1–2 months during which he had more frequent infusions. Histopathologic review at the NIH revealed a grade 3/3 papillary transitional cell carcinoma invading the muscularis propria. Now, 9 years after diagnosis, the patient is in good health with no symptoms of recurrence or metastasis. The patient used the following supplements: botanical extract, chondroitin sulfate, chromium picolinate, flax oil, glucosamine sulfate, α-lipoic acid, Lactobacillus acidophilus and L. rhamnosus and selenium (Table 2).
Complete or partial bladder removal is the standard treatment for stage T2 (muscle invasive) bladder cancer, since the presence of muscle invasion appears to be the best predictor of aggressive behaviour. When treated only locally, as in this case, invasive transitional cell bladder cancer almost invariably develops into clinically apparent local or metastatic disease within a short period.33–35 There are reports of transurethral tumour resection being offered as the sole initial therapy in carefully selected patients with T2 disease. In one report 20% of patients with muscle invasive bladder cancer treated only with transurethral resection remained free of recurrent disease after 3–7 years of follow-up.36 However, such minimal therapy is considered an option only when the cancer is solitary, well defined and completely excised as documented by pathologic evaluation,37 whereas this patient presented with multiple tumours and associated muscle invasion.
Patient 3
This case was previously reported but without detail and without independent pathologic confirmation.26,30 A 66-year-old woman was found in January 1995 to have a large left paraspinal mass medial to the iliopsoas muscle at the L4–5 level. On imaging the mass measured 3.5–7 cm transversely and 11 cm in the craniocaudal direction, with evidence of extension into the posterior paraspinal muscle and bone invasion. Chest radiography results were normal. An open biopsy specimen was diagnostic of a diffuse large B-cell lymphoma. The patient's oncologist recommended local radiation therapy and chemotherapy. Although she agreed to a 5-week course of local radiation therapy, the patient refused chemotherapy, electing instead to receive vitamin C intravenously. She received 15 g of vitamin C twice per week for about 2 months, 15 g once to twice per week for about 7 months, and then 15 g once every 2–3 months for about 1 year. This began in mid-January 1995 concurrently with the radiation therapy, which was given as AP/PA parallel opposed 18 MEV x-rays and between 1–18 and 2–28–95, 5040 Centi Gray in 28 fractions delivered to the mid-plane of the body with 3:2 loading from the back. At this time a left axillary lymph node 1 cm in diameter and a right axillary lymph node 1.5 cm in diameter were palpable.
Two weeks later, in early February 1995, the right and left axillary lymph nodes remained palpable and a new left cervical lymph node 1 cm in diameter and a new left supraclavicular lymph node larger than 1 cm were apparent on physical examination. Intravenous vitamin C therapy continued. Three weeks later the supraclavicular and cervical lymph nodes were no longer palpable, the left axillary node had disappeared, and the right axillary node had decreased in size to less than 1 cm. After a further 3 weeks, in mid-March 1995, there was no lymphadenopathy in the neck and no palpable axillary lymphadenopathy. In late April 1995 a new left cervical lymph node was detected, and histopathologic review identified a biopsy specimen as identical to the original tumour. The patient once again refused chemotherapy and continued her program of intravenous vitamin C injections. Two months later, in June 1995, there was marked left supraclavicular lymphadenopthy 3 cm in size, with shotty right axillary nodes but no adenopathy in the left axilla. Four months later, in October 1995, a single right submandibular node was palpable, but the supraclavicular and all other areas, including the axillas, had no palpable lymph nodes. In May 1996 a left anterior cervical node 1.5 cm in size was present, but there was no other adenopathy. Intravenous vitamin C therapy continued through late December 1996, at which time the patient was in normal health and had no clinical sign of lymphoma. The patient remains in normal health 10 years after the diagnosis of diffuse large B-cell lymphoma, never having received chemotherapy. The patient used additional products: β-carotene, bioflavonoids, chondroitin sulfate, coenzyme Q10, dehydroepiandrosterone, a multiple vitamin supplement, N-acetylcysteine, a botanical supplement and bismuth tablets (Table 3). Histopathologic examination of the original paraspinal mass at the NIH confirmed a diffuse large B-cell lymphoma at stage III, with a brisk mitotic rate.
Patients with untreated stage III diffuse B-cell lymphoma have a dismal prognosis. This case, like the preceding one, is unusual in that the patient refused chemotherapy, which might have produced a long-term remission. It appears, nonetheless, that a cure occurred in connection with intravenous vitamin C infusions.
Discussion
These cases were analyzed in accordance with the NCI's Best Case Series process, which reports and interprets apparent responses to alternative therapies.23,24 Apart from its implications regarding vitamin C, this article illustrates the use of the Best Case Series approach in assessing the clinical plausibility of novel therapies. None of these case histories provides definitive proof that intravenous vitamin C therapy was responsible for the patient's unusually favourable clinical course. It is often difficult to prove definitively that a given treatment is responsible for a specific clinical outcome. When the treatment is unorthodox, alternative explanations, even if highly unlikely, tend to be preferred.38,39 However, although they do not provide grounds for advocating intravenous vitamin C therapy as a cancer treatment, these cases increase the clinical plausibility of the notion that vitamin C administered intravenously might have effects on cancer under certain circumstances.
The overall plausibility of ascorbic acid administered intravenously as a cancer therapy is enhanced by recent insights into clinical pharmacokinetics and in vitro cancer-specific cytotoxicity of vitamin C.15–20Pharmacokinetics data show that orally administered vitamin C results in tightly controlled plasma and cell concentrations. Subjects consuming 200–300 mg per day of vitamin C in 5 or more daily servings of fruits and vegetables have fasting steady state plasma concentrations of about 70–80 μmol/L.40,41 Even with maximally tolerated oral doses of 3 g every 4 hours, peak plasma concentrations are estimated to not exceed 220 μmol/L.15 Intravenous administration of vitamin C bypasses tight control for several hours, until homeostasis is restored by renal excretion. Depending on the dose and infusion rate, peak plasma concentrations obtained intravenously are estimated to reach 14 000 μmol/L, and concentrations above 2000 μmol/L may persist for several hours. Emerging in vitro data show that extracellular ascorbic acid selectively kills some cancer but no normal cells by generating hydrogen peroxide.20 Death is mediated exclusively by extracellular ascorbate, at pharmacologic concentrations that can be achieved only by intravenous administration. Vitamin C may serve as a pro-drug for hydrogen peroxide delivery to extravascular tissues, but without the presence of hydrogen peroxide in blood. These data are consistent with clinical pharmacokinetics of vitamin C administered intravenously.15 Of note, only a minority of cancer patients reported by Cameron and colleagues responded to intravenous and oral vitamin C therapy,1–4 and not all cancer cells were killed by ascorbic acid in vitro.20 Further basic investigation of pharmacologic vitamin C concentrations in mediating cell death will facilitate discovery of the mechanisms responsible for sensitivity and resistance in vitro and in vivo. On the basis of emerging clinical and in vitro data, early-phase clinical trials of intravenous vitamin C therapy alone and in combination with conventional chemotherapy are currently in the planning and execution phase, including a formal phase I trial in progress at McGill University.42–44
The cases reported here do not prove that vitamin C induced the favourable outcomes observed. These patients received other alternative medicine therapies. Spontaneous remission of some tumours may occur rarely, although the 3 cancers reported here are dissimilar. Accretion of more cases meeting NCI Best Case Series guidelines may indicate whether vitamin C or other factors contribute to such remissions.
It is likely that high vitamin C intakes have low toxicity, except under certain conditions.45,46 Intravascular hemolysis was reported after massive vitamin C administration in people with glucose-6-phosphate dehydrogenase deficiency.46 Administration of high-dose vitamin C to patients with systemic iron overload may increase iron absorption and represents a contraindication.46,47 Ascorbic acid is metabolized to oxalate, and 2 cases of acute oxalate nephropathy were reported in patients with pre-existing renal insufficiency given massive intravenous doses of vitamin C.48,49 Therefore, patients with renal insufficiency or renal failure, or who are undergoing dialysis, should not receive high doses of vitamin C.46It is controversial whether high-dose vitamin C use is associated with oxalate kidney stones, and patients with hyperoxaluria or a prior history of oxalate kidney stones have a relative contraindication to high-dose vitamin C.46 Rare cases of acute tumour hemorrhage and necrosis were reported in patients with advanced cancer within a few days of starting high-dose intravenous vitamin C therapy, although this was not independently verified by pathologic review.1,50 Although tumour hemorrhage suggests an anticancer potential for ascorbate, there is the potential for risk to some patients.
The cases reported here are of tumours confirmed by histopathologic examination to have poor prognosis but that instead had long clinical remissions. Most previous case reports lacked independent pathologic confirmation of the tumour and did not follow the NCI Best Case Series guidelines, which makes their interpretation difficult. Recent findings show that only high-dose intravenous, but not oral, vitamin C therapy results in very high plasma vitamin C concentrations (e.g., 14 000 μmol/L). At these concentrations, the vitamin is toxic to some cancer cells, possibly because at these concentrations the vitamin is a pro-drug for hydrogen peroxide formation in extracellular fluid. Accumulated data confer some degree of biological and clinical plausibility to the notion that high-dose intravenous vitamin C therapy may have anti-tumour effects in certain cancers. When all available data are considered, further clinical study as to safety and efficacy of intravenous vitamin C is warranted.





This site summarises three cases of IV Vitamin C administration with dosages used in each case: Intravenously administered vitamin C as cancer therapy: three cases
I wanted to add this but it was too late to edit my post: I'll see if I can find some successful and unsuccessful stories and check whether there is a notable difference in dosages. As mentioned above, diet is a likely factor behind both success and failure stories so I'll see if I can pick up some patterns.
A specific protocol and variations of it are mentioned here with tables that show how it was diluted:
https://www.researchgate.net/public...bic_acid_protocol_for_its_application_and_use
At the bottom of the follwoing article is "The Riordian IVC Protocol". Also very detailed with tables and such:
Edit: This one was already mentioned above: see here.
https://www.researchgate.net/public...bic_acid_protocol_for_its_application_and_use
At the bottom of the follwoing article is "The Riordian IVC Protocol". Also very detailed with tables and such:
Edit: This one was already mentioned above: see here.
Last edited:
This one provides lots of data and dosages: IVC Protocol Vitamin C Research | Riordan Clinic
ADDED: I'm sorry for the duplicate Pashalis! I only noticed it's the same link you provided after I posted mine.
ADDED: I'm sorry for the duplicate Pashalis! I only noticed it's the same link you provided after I posted mine.
Vitamin C (ascorbate, ascorbic acid) is a major water-soluble antioxidant that also increases extracellular collagen production and is important for proper immune cell functioning (Hoffman, 1985; Cameron, et al., 1979). It also plays key roles in L-carnitine synthesis, cholesterol metabolism, cytochrome P-450 activity, and neurotransmitter synthesis (Geeraert, 2012). The Riordan intravenous vitamin C (IVC) protocol involves the slow infusion of vitamin C at doses on the order of 0.1 to 1.0 grams ascorbate per kilogram body mass (Riordan, et al., 2003). IVC use has increased recently among integrative and orthomolecular medicine practitioners: a survey of roughly 300 practitioners conducted between 2006 and 2008 indicated that roughly ten thousand patients received IVC, at an average dose of 0.5 g/kg, without significant ill effects (Padayatty, et al., 2010). While IVC may have a variety of possible applications, such as combating infections (Padayatty, et al., 2010), treating rheumatoid arthritis (Mikirova, et al., 2012), it has generated the most interest for its potential use in adjunctive cancer care.
Vitamin C was first suggested as a tool for cancer treatment in the 1950′s: its role in collagen production and protection led scientists to hypothesize that ascorbate replenishment would protect normal tissue from tumor invasiveness and metastasis (McCormick, 1959; Cameron, et al., 1979). Also, since cancer patients are often depleted of vitamin C (Hoffman, 1985; Riordan, et al., 2005), replenishment may improve immune system function and enhance patient health and well-being (Henson, et al., 1991). Cameron and Pauling observed fourfold survival times in terminal cancer patients treated with intravenous ascorbate infusions followed by oral supplementation (Cameron & Pauling, 1976). However, two randomized clinical trials with oral ascorbate alone conducted by the Mayo clinic showed no benefit (Creagan, et al., 1979; Moertel, et al., 1985). Most research from that point on focused on intravenous ascorbate. The rationales for using intravenous ascorbate infusions (IVC) to treat cancer, which are discussed in detail below, can be summarized as follows:
- Plasma ascorbate concentrations in the millimolar range can be safely achieved with IVC infusions.
- At millimolar concentrations, ascorbate is preferentially toxic to cancer cells in vitro and is able to inhibit angiogenesis in vitro and in vivo.
- Vitamin C can accumulate in tumors, with significant tumor growth inhibition seen (in guinea pigs) at intra-tumor concentrations of 1 mM or higher.
- Published case studies report anti-cancer efficacy, improved patient well-being, and decreases in markers of inflammation and tumor growth.
- Phase I clinical studies indicate that IVC can be administered safely with relatively few adverse effects.
Types of cancers treated with IVC by the Riordan clinic:
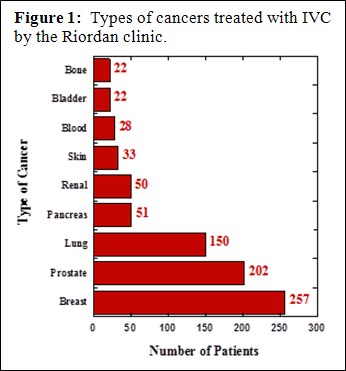
The Riordan clinic has treated hundreds of cancer patients (Figure 1) using the Riordan protocol. At the same time, Riordan Clinic Research Institute (RCRI) has been researching the potential of intravenous vitamin C therapy for over thirty years. Our efforts have included in vitro studies, animal studies, pharmacokinetic analyses, and clinical trials. The Riordan IVC protocol, along with the research results (by the RCRI and others) that have motivated its use, is described below.
SCIENTIFIC BACKGROUND
Pharmacokinetics
Vitamin C is water-soluble, and is limited in how well it can be absorbed when given orally. While ascorbate tends to accumulate in adrenal glands, the brain, and in some white blood cell types, plasma levels stay relatively low (Hornig, 1975; Keith & Pelletier, 1974; Ginter, et al., 1979; Kuether, et al., 1988). Data by Levine and coworkers indicate that plasma levels in healthy adults stayed below 100 µM, even if 2.5 grams were taken when administered once daily by the oral route. (Levine, et al., 1996).
Cancer patients tend to be depleted of vitamin C: fourteen out of twenty-two terminal cancer patients in a phase I study we depleted of vitamin C, with ten of those having zero detectable ascorbate in their plasma (Riordan, et al., 2005). This is shown in Figure 2. In a study of cancer patients in hospice care, Mayland and coworkers found that thirty percent of the subjects were deficiency in vitamin C (Mayland, et al., 2005). Deficiency (below 10 µM) was correlated with elevated CRP (c-reactive protein, an inflammation marker) levels and shorter survival times. Given the role of vitamin C in collagen production, immune system functioning, and antioxidant protection, it is not surprising that subjects depleted of ascorbate would fare poorly in mounting defenses against cancer. This also suggests that supplementation to replenish vitamin C stores might serve as adjunctive therapy for these patients.
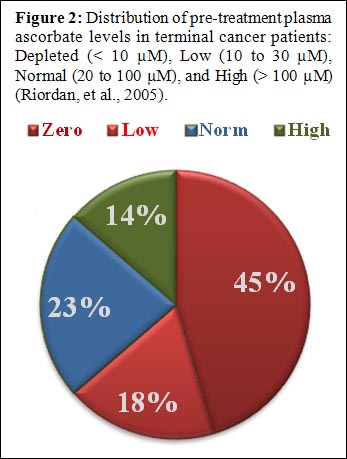
Figure 2: Distribution of pre-treatment plasma ascorbate levels in terminal cancer patients: Depleted (< 10 µM), Low (10 to 30 µM), Normal (20 to 100 µM), and High (> 100 µM) (Riordan, et al., 2005).
When vitamin C is given by intravenous infusion, peak concentrations over 10 mM can be attained (Casciari, et al., 2001; Padayatty, et al., 2004) without significant adverse effects to the recipient. Figure 3 shows plasma ascorbate concentrations attained via IVC infusion at the Riordan Clinic, while Figure 4 shows pharmacokinetic data for two subjects given eighty minute IVC infusions. These peak plasma concentrations are two orders of magnitude above what is observed with oral supplementation. This suggests that IVC may be more effective than oral supplementation in restoring depleted ascorbate stores in cancer patients. Physicians at the Riordan Clinic have observed that (a) peak plasma concentrations attained after IVC infusions tend to be lower in cancer patients than in healthy volunteers, suggesting their depleted tissues act as a “sink” for the vitamin; and (b) in cancer patients given multiple IVC treatments, baseline plasma ascorbate concentrations tend to increase to normal levels slowly over time as reserves are restored with adequate IVC dosing.
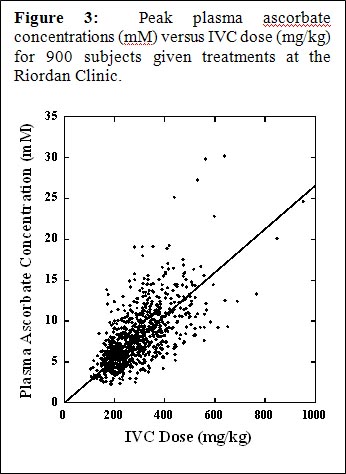
Figure 3: Peak plasma ascorbate concentrations (mM) versus IVC dose (mg/kg) for 900 subjects given treatments at the Riordan Clinic.
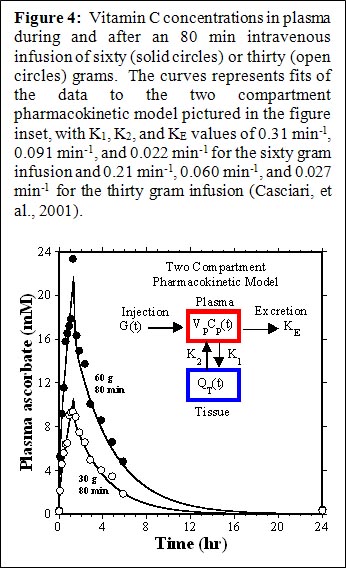
Figure 4: Vitamin C concentrations in plasma during and after an 80 min intravenous infusion of sixty (solid circles) or thirty (open circles) grams. The curves represents fits of the data to the two compartment pharmacokinetic model pictured in the figure inset, with K1, K2, and KE values of 0.31 min-1, 0.091 min-1, and 0.022 min-1 for the sixty gram infusion and 0.21 min-1, 0.060 min-1, and 0.027 min-1 for the thirty gram infusion (Casciari, et al., 2001).
In addition to providing ascorbate replenishment, IVC may allow oncologists to exploit some interesting anti-cancer properties, including high dose IVC’s ability to induce tumor cell apoptosis, inhibit angiogenesis, and reduce inflammation. In vitro and in vivo data supporting these potential mechanisms of action, discussed below, suggest that they may be relevant at ascorbate concentrations on the order of 2 mM. As shown in Figures 3 and 4, these concentrations are attainable in plasma using progressive dosing of IVC. A 2-compartment model can be used to predict peak and “average” (over 24 hours) plasma ascorbate concentrations for an average sized adult at a given IVC dose. This calculation suggests that a 50 gram, 1 hr. infusion would yield a peak plasma concentration of roughly 18 mM and an integral average of roughly 2.6 mM, a reasonable target for producing anti-cancer effects.

Figure 5: Target IVC dose based on attaining a high enough integral average ascorbate concentration (24 hr) for anti-cancer effects.
Peroxide-based Cytotoxicity
Vitamin C, at normal physiological concentrations (0.1 mM), is a major water-soluble antioxidant (Geeraert, 2012). At concentrations on the order of 1 mM, however, continuous perfusion of ascorbate at doses that trigger “redox cycling” can cause a build-up of hydrogen peroxide, which is preferentially toxic toward tumor cells (Benade, et al., 1969; Riordan, et al., 1995; Casciari, et al., 2001; Chen, et al., 2005; Frei & Lawson, 2008), often leading to autophagy or apoptosis. To examine this cytotoxic effect in a three dimensional model, the RCRI employed hollow-fiber in vitro solid tumors (HFST). Figure 6 shows a histological section of colon cancer cells growing in this configuration. Dual staining annexin V and propidium iodide flow cytometry showed as significant increase in apoptosis, along with decreased surviving fractions, at ascorbate concentrations in the 1 mM to 10 mM range. Ascorbate concentrations required for toxicity in the HFST model (LC50 = 20 mM), with only two days incubation, were much higher than those typically observed in cell monolayers. The cytotoxic threshold could be reduced significantly (LC50 = 4 mM) by using ascorbate in combination with alpha-lipoic acid. Other reports suggest that ascorbate cytotoxicity against cancer cells can be increased by using it in combination with menadione (Verrax, et al., 2004) or copper containing compounds (Gonzalez, et al., 2002).
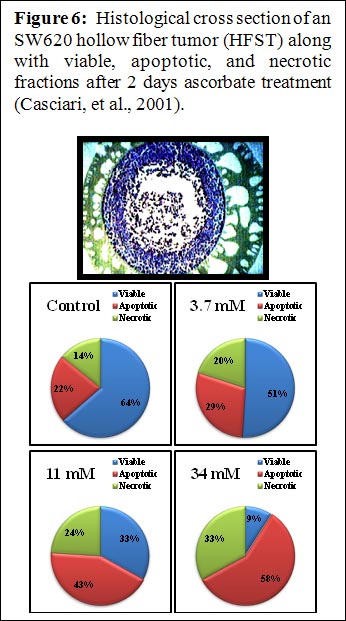
IVC-Protocol-Vitamin-C-Research-Riordan-Clinic-Hollow-Fiber-Tumor
Figure 6: Histological cross section of an SW620 hollow fiber tumor (HFST) along with viable, apoptotic, and necrotic fractions after 2 days ascorbate treatment (Casciari, et al., 2001).
Studies from many laboratories in a variety animal models, using hepatoma, pancreatic cancer, colon cancer, sarcoma, leukemia, prostate cancer, and mesothelioma confirm that ascorbate concentrations sufficient for its cytotoxicity can be attained in vivo, and that treatments can reduce tumor growth (Chen, et al., 2008; Verrax & Calderon, 2009; Du, et al., 2010; Belin, et al., 2009; Yeom, et al., 2009; Pollard, et al., 2010). Figure 7 shows data using the L-10 model in guinea pigs. L 10 tumor cells implanted subcutaneously metastasize to the lymph nodes. The overall tumor burden (primary plus metastases) was then determined after 30 days of tumor growth and 18 days of ascorbate therapy. Note that here the actual intra-tumor ascorbate concentrations were measured, and the correlation between tumor mass and tumor ascorbate concentration is strong regardless of the mode of ascorbate administration. The precentage of tumor growth inhibition, relative to controls, was roughly 50% at intra-tumor ascorbate concentrations of 1 mM tumor and roughly 65% once the intra-tumor ascorbate level went above 2 mM. The ascorbate dosage used in this study was 500 mg/kg/day. Our scientists also looked at survival times of BALP/C mice with S180 sarcomas. The results are shown in Figure 8. The median survival time for the untreated mice was 35.7 days post implantaion, while that for ascorbate treated mice (700 mg/kg/day) was 50.7 days. Of course, the efficacy observed in these animal studies may be due to some combination of direct cytotoxicity and other factors, such as angiogenesis inhibition (Yeom, et al., 2009) or other biological response modifications (Cameron, et al., 1979).
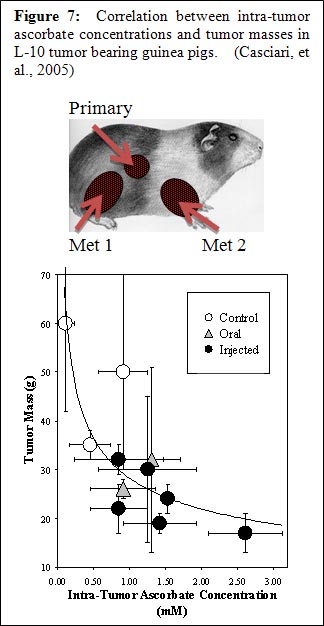
Figure 7: Correlation between intra-tumor ascorbate concentrations and tumor masses in L-10 tumor bearing guinea pigs. (Casciari, et al., 2005)
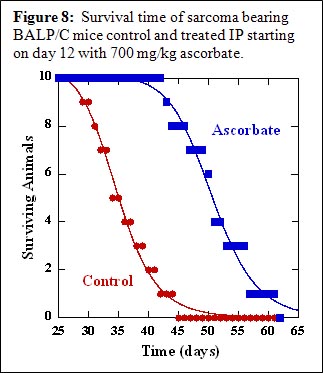
Figure 8: Survival time of sarcoma bearing BALP/C mice control and treated IP starting on day 12 with 700 mg/kg ascorbate.
Angiogenesis Inhibition
Tumor angiogenesis is the process of new blood vessel growth toward and into a tumor. It is considered to be critical in tumor growth and metastasis. Reports in the literature suggst that ascorbate’s effect on collagen synthesis can act to inhibit formation of new vascular tubules (Ashino, et al., 2003), that ascorbate can inhibit genes necessary for angiogenesis (Berlin, et al., 2009), and that it might influence angiogenesis through its effect on hypoxia inducable factor (Page, et al., 2007).
The Riordan clinic researchers evaluated angiogenesis inhibition using four different experimental models. In all cases, there is an inhibitory effect on angiogenesis at ascorbate concentrations of 1 to 10 mM (Mikirova, et al., 2008; Mikirova, et al., 2012).
- The growth of new micro-vessels from aortic rings ex vivo is inhibited by ascorbate at concentration 5 mM of more, as shown in Figure 9.
- Ascorbate inhibits endothelial cell tubule formation in Matrigel in vitro in a concentration dependent fashon. Number of intact tubule loops was decreased by half at concentrations of 11 mM for endothelial progenitor cells and 17 mM for HUVEC cells.
- The rate at which endothelial cells can migrate on a petri dish to fill a gap between them was reduced when 5.7 mM ascorbate was added after the gap was created. The asocrbate also reduced ATP production in these endothelial cells by twenty perceont, but did not affect cell viability.
- Restores appropriate nerve function
- For Matrigel plugs implanted subcutaneously in mice, the micro-vessel density we significantly lower in mice treated with 430 mg/kg every other day for two weeks.
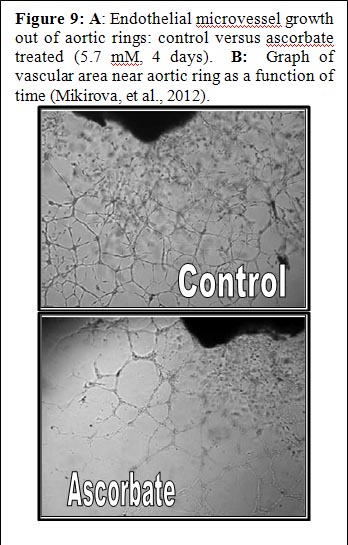
Figure 9 A): Endothelial microvessel growth out of aortic rings: control versus ascorbate treated (5.7 mM, 4 days).
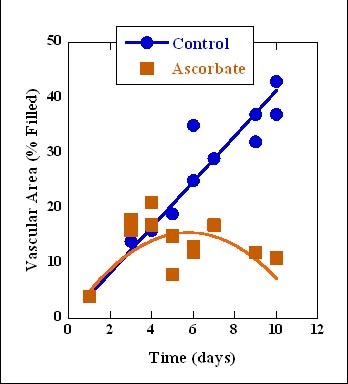
Figure 9 B): Graph of vascular area near aortic ring as a function of time (Mikirova, et al., 2012).
In animal experiments and clinical case studies where high ascorbate doses show efficacy against tumors, this benefit may represent therapeutic synergism due to both angiogenesis inhibition as well as to direct cytotoxicity or other causes.
Inflammation Modulation
Analysis of clinical data from the Riordan Clinic suggests that inflammation is an issue for cancer patients, and that it can be lessened during IVC therapy (Mikirova, et al., 2012). C-reactive protein was used as a marker of inflammation, as reports in the literature indicate that elevated CRP is correlated with poor patient prognosis (St. Sauver, et al., 2009). Over sixty percent of analyzed Riordan Clinic cancer patients had CRP levels above 10 mg/L prior to IVC therapy. In 76 ± 13% of these subjects, IVC reduced CRP levels. This improvement was more prevalent, 86 ± 13%, in subjects with elevated (above 10 mg/L) CRP. Comparisons of individual values before and after treatments are shown in Figure 10A. Since many of the subjects in this database were prostate cancer patients, we examined prostate specific antigen (PSA) levels before and after therapy. This is shown in Figure 10B. Most of the prostate cancer patients showed reductions in PSA levels during the course of their IVC therapy. This was not true with other markers, as shown in Figure 10C. In some subjects, both tumor marker and CRP data were available both before and after IVC therapy. In those cases, there was a strong correlation (r2 = 0.62) between the change in tumor marker and the change in CRP during IVC therapy. This is consistent with observations from the literature showing a correlation between CRP levels and PSA levels in prostate cancer patients (Lin, et al., 2010).
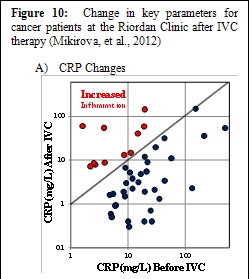
Figure 10 A): Endothelial microvessel growth out of aortic rings: control versus ascorbate treated (5.7 mM, 4 days)
A) CRP Changes
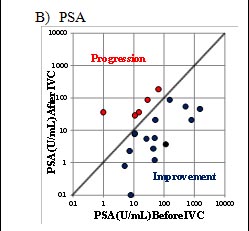
Figure 10 B): Endothelial microvessel growth out of aortic rings: control versus ascorbate treated (5.7 mM, 4 days)
B) PSA
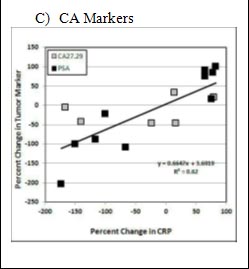
Figure 10 C): Endothelial microvessel growth out of aortic rings: control versus ascorbate treated (5.7 mM, 4 days)
C) CA Markers
The potential effect of IVC in reducing inflammation is also supported by cytokine data: serum concentrations of the pro-inflammatory cytokines IL-1α, IFN-γ, IL-8, IL-2, TNF-α and eotaxin were acutely reduced after a fifty gram ascorbate infusion, and in the case of the last three cytokines listed, reductions were maintained throughout the course of IVC therapy (Mikirova, et al., 2012).
Inflammation Modulation
The observations that ascorbate is an antioxidant and that it preferentially accumulates in tumors (Agus, et al., 1999) have raised fears that ascorbate supplementation would compromise the efficacy of chemotherapy (Raloff, 2000). In support of this, Heaney and coworkers found that tumor cells in vitro and xenografts in mice were more resistant to a variety of anticancer agents when the tumor cells were pretreated with dehydroascorbic acid (Heaney, et al., 2008). Questions have been raised, however, whether the experimental conditions used in the Heaney study are clinically or biochemically relevant, considering, among other issues, that dehydroascorbic acid rather than ascorbic acid was used (Espey, et al., 2009). It should also be noted that the goal of IVC is to attain millimolar intra-tumor concentrations (for the reasons described above) and thus the accumulation of ascorbate in tumors is considered an advantage.
A variety of laboratory studies suggest that, at high concentrations, ascorbate does not interfere with chemotherapy or irradiation and may enhance efficacy in some situations (Fujita, et al., 1982; Okunieff & Suit, 1987; Kurbacher, et al., 1996; Taper, et al., 1996; Fromberg, et al., 2011; Shinozaki, et al., 2011; Espey, et al., 2011). This is supported by meta-analyses of clinical studies involving cancer and vitamins; these studies conclude that antioxidant supplementation does not interfere with the toxicity of chemotherapeutic regiments (Simone, et al., 2007; Block, et al., 2008).
CLINICAL DATA
Case Studies
The situation with intravenous ascorbate therapy is different from that with new chemotherapeutic agents in that FDA approval was not strictly required in order for physicians to administer IVC. As a result, clinical investigations tended to run concurrently with laboratory research. Two early studies indicated that intravenous ascorbate therapy could increase survival times beyond expectations in cancer patients (Cameron & Pauling, 1976; Murata, et al., 1982). There have been several case studies published by the Riordan Clinic team (Jackson, et al., 1995; Riordan, et al., 1998; Riordan, et al., 1996) and collaborators (Padayatti, et al., 2006; Drisko, et al., 2003). While these case studies do not represent conclusive evidence in the same way that a well-designed Phase III study would, they are nonetheless of interest for comparing methodologies and motivating future research, in addition to being of monumental importance to the individuals who were their subjects. Some key case studies are summarized here:
- 51 year old female with renal cell carcinoma (nuclear grade III/IV) and lung metastasis declined chemotherapy and instead chose to intravenous ascorbate at an initial dose of 15 grams. Her dose was increased to 65 grams after two weeks. She continued at this dose for ten months. Patient received no radiation or chemotherapy. The patient supplemented with thymus protein extract, N-acetylcysteine, niacinamide, beta-glucan, and thyroid extract. Seven of eight lung masses resolved. Patient went four years without evidence of regression. Four years later, patient showed a new mass (consistent with small-cell lung cancer, not with recurrent renal carcinoma metastasis) and died shortly afterward (Padayatti, et al., 2006).
- A 49 year old male with a bladder tumor (invasive grade 3/3 papillary transitional cell carcinoma) and multiple satellite tumors declined chemotherapy and instead chose to receive intravenous ascorbate. He received 30 grams twice weekly for three months, followed by 30 grams monthly for four years. Patient supplementation included botanical extract, chondroitin sulfate, chromium picolinate, flax oil, glucosamine sulfate, alpha-lipoic acid, lactobacillus acidophilus, L. rhamnosus, and selenium. Nine years after the onset of therapy, patient is in good health with no signs of recurrence or metastasis (Padayatti, et al., 2006).
- A 66 year old woman with diffuse Stage III large B-cell lymphoma with a brisk mitotic rate and large left paraspinal mass (3.5 – 7 cm transverse and 11 cm craniocaudal) showing evidence of bone invasion agreed to a five-week course of radiation therapy, but refused chemotherapy and instead chose to receive intravenous ascorbate concurrent with radiation. She received 15 grams twice weekly for two months, once per week for seven months, and then once every two-three months for one year. Patient supplementation included coenzyme Q10, magnesium, beta-carotene, parasidal, vitamin B and C supplements, Parex and n-acetylcysteine. The original mass remained palpable after radiation therapy and a new mass appeared. Vitamin C therapy continued. Six weeks later, masses were not palpable. A new lymph mass was detected after four months, but the patient showed no clinical signs of lymphoma after one year. Ten years diagnosis, the patient remained in normal health (Padayatti, et al., 2006).
- A 55 year old woman with stage IIIC papillary adenocarcinoma of the ovary and an initial CA-125 of 999 underwent surgery followed by six cycles of chemotherapy (paclitaxel, carboplatin) combined with oral and parenteral ascorbate. Ascorbate infusion began at 15 grams twice weekly and increased to 60 grams twice weekly. Plasma ascorbate levels above 200 mg/dL were achieved during infusion. After six weeks, ascorbate treatment continued for one year, after which patient reduced infusions to once every two weeks. The patient also supplemented with vitamin E, coenzyme Q10, vitamin C, beta-carotene, and vitamin A. At the time of publication, she was over 40 months from initial diagnosis and remained on ascorbate infusions. All CT and PET scans were negative for disease, and her CA-125 levels remained normal (Drisko, et al., 2003).
- A 60 year old woman with stage IIIC adenocarcinoma of the ovary and an initial CA-125 of 81 underwent surgery followed by six cycles of chemotherapy (paclitaxel, carboplatin) with oral antioxidants. After six cycles of chemotherapy, patient began parenteral ascorbate infusions. Ascorbate infusion began at 15 grams once weekly and increased to 60 grams twice weekly. Plasma ascorbate levels above 200 mg/dL were achieved during infusion. Treatment continued to date of publication. The patient supplemented with vitamin E, coenzyme Q10, vitamin C, beta-carotene, and vitamin A. Her CA-125 levels normalized after one course of chemotherapy. After the first cycle of chemotherapy, the patient was noted to have residual disease in the pelvis. At this point, she opted for intravenous ascorbate. Thirty months later, patient showed no evidence of recurrent disease and her CA-125 levels remained normal.
- Note that these case studies involve a variety of cancer types, sometimes involve the use of IVC in conjunction with chemotherapy or irradiation, and usually involve the use of other nutritional supplements by the subject.
Several other clinical studies looked into the effect of vitamin C on quality of life in cancer patients. In a Korean study, IVC therapy significantly improved global quality of life scores, with benefits including less fatigue, reduction in nausea and vomiting, and improved appetite (Yeom, et al., 2007). In a recent German study, breast cancer patients receiving IVC along with standard therapy were compared to subjects receiving standard therapy alone (Vollbracht, et al., 2011). Patients given IVC benefited from less fatigue, reduction in nausea, improved appetite, reductions in depression and fewer sleep disorders. Overall intensity scores of symptoms during therapy and aftercare was twice as high in the control group as the IVC group. No side effects due to ascorbate were observed, nor were changes in tumor status compared to controls reported.
Phase I Clinical Trials
he safety of intravenous ascorbate has been addressed in recently published Phase I clinical studies (Riordan, et al., 2005; Hoffer, et al., 208; Monti, et al., 2012). The first Phase I study was conducted with twenty-four terminal cancer patients (mostly liver and colorectal cancers) (Riordan, et al., 2005). The study used doses up to 710 mg/kg/day. Figure 11 shows how parameters associated with renal function changed during the course of treatment. These indicators remained steady or decreased over time; this is significant since they would be expected to rise during treatment if ascorbate was having an acute detrimental effect on renal function. Blood chemistries suggested no compromise in renal function, and one patient showed stable disease, continuing treatment for an additional 48 weeks. Adverse effects reported were mostly minor (nausea, edema, dry mouth or skin). Two grade three adverse events “possible related” to the agent were reported: a kidney stone in a patient with a history of renal calculus and a patient who experienced hypokalemia. These patients were generally vitamin C deficient at the start of treatment, and plasma ascorbate concentrations did not exceed 3.8 mM.
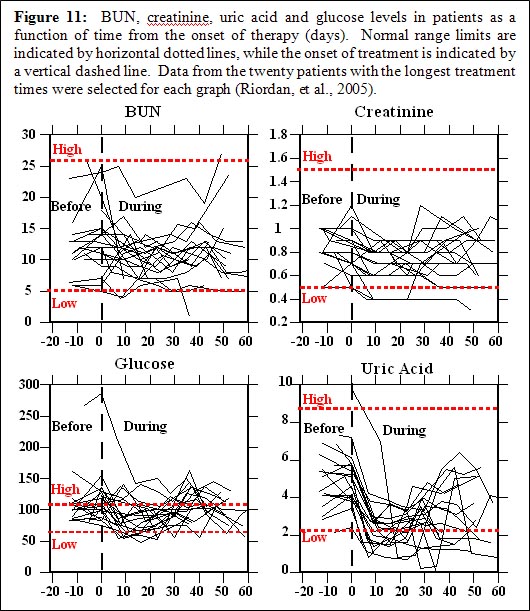
Figure 11: BUN, creatinine, uric acid and glucose levels in patients as a function of time from the onset of therapy (days). Normal range limits are indicated by horizontal dotted lines, while the onset of treatment is indicated by a vertical dashed line. Data from the twenty patients with the longest treatment times were selected for each graph (Riordan, et al., 2005).
In the study by Hoffer and coworkers (Hoffer, et al., 208), twenty-four subjects with advanced cancer or hematologic malignancy not amenable to standard therapy were given IVC at doses of 0.4 g/kg to 1.5 g/kg (equivalent to a range of 28 to 125 grams in a 70 kg adult) three times weekly. In this study, peak plasma concentrations in excess of 10 mM were obtained, and no serious side effects were reported. Subjects at higher doses maintained physical quality of life, but no objective anti-cancer response was reported. The study by Monti and coworkers (Monti, et al., 2012), fourteen patients received IVC in addition to nucleoside analogue gemcitabine and the tyrosine kinase inhibitor erlotinib. Observed adverse events were attributable to the chemotherapeutic agents, but not to the ascorbate, but no added efficacy due to the ascorbate was observed.
Thus far, Phase I studies indicate that IVC can be safely administered to terminal cancer patients at high doses (10 to 100 grams or more), but anti-cancer efficacy of the sort reported in case studies has not yet been observed. Of course, the terminal subjects used in Phase I studies would be expected to be the most difficult to treat. Phase II studies, with longer durations, are needed at this point.
Safety Issues Reported In Literature
Evidence indicates that patients who show no prior signs or history of renal malfunction are unlikely to suffer ill effects to their renal systems as a result of intravenous ascorbate (Riordan, et al., 2005). In cases where there are preexisting renal problems, however, caution is advised. In addition a kidney stone forming in one patient with a history of stone formation (Riordan, et al., 2005), a patient with bilateral urethral obstruction and renal insufficiency suffered acute oxalate neuropathy (Wong, et al., 1994). A full blood chemistry and urinalysis work-up is thus recommended prior to the onset of intravenous ascorbate therapy.
Campbell and Jack (Campbell & Jack, 1979) reported that one patient died due to massive tumor necrosis and hemorrhaging following an initial dose of intravenous ascorbate. It is thus recommended that treatment start at a low dose and be carried out using slow “drip” infusion. Fatal Hemolysis can occur if a patient has glucose-6-phosphate dehydrogenase deficiency. It is thus recommended that G6PD levels be assessed prior to the onset of therapy. The treatment is contra-indicated in situations where increased fluids, sodium, or chelating may cause serious problems. These situations include congestive heart failure, edema, ascites, chronic hemodialysis, unusual iron overload, and inadequate hydration or urine void volume (Rivers, 1987).
THE RIORDAN IVC PROTOCOL
Inclusion Criteria and Candidates
- Candidates include those who have failed standard treatment regimens; those seeking to improve the effectiveness of their standard cancer therapy; those seeking to decrease the severity and carcinogenicity of side effects from standard cancer therapy; those attempting to prolong their remission with health-enhancing strategies; those declining standard treatment, yet wishing to pursue primary, alternative treatment.
- Patient (guardian or legally recognized care-giver) must sign a consent-to-treat or release form for the IVC treatment. Patient should have no significant psychiatric disorder, end-stage CHF, or other uncontrolled co-morbid conditions.
- Obtain baseline and screening laboratory:
- Serum chemistry profile with electrolytes
- Complete blood count (CBC) with differential
- Red blood cell G6PD (must be normal)
- Complete urinalysis
- In order to properly assess the patient’s response to IVC therapy, obtain complete patient record information prior to beginning IVC therapy:
- Tumor type and staging, including operative reports, pathology reports, special procedure reports, and other staging information. (Re-staging may be necessary if relapse and symptom progression has occurred since diagnosis.)
- Appropriate tumor markers, CT, MRI, PET scans, bone scans, and x-ray imaging.
- Prior cancer treatments, the patient’s response to each treatment type, including side effects.
- The patient’s functional status with an ECOG Performance Score.
- Patient weight.
- Precautions and Side Effects
In the Riordan Clinic’s experience giving over 40,000 onsite IVC treatments, the side-effects of high-dose IVC are rare. However, there are precautions and potential side-effects to consider.
- The danger of diabetics on insulin incorrectly interpreting their glucometer finger stick has been found. It is important to notice to health care workers using this protocol for the treatment of cancer in patients who are also diabetic: high dose intravenous vitamin C (IVC) at levels 15 grams and higher will cause a false positive on finger-stick blood glucose strips (electrochemical method) read on various glucometers (Jackson & Hunninghake, 2006). Depending on the dose, the false positive glucose and occasionally “positive ketone” readings may last for eight hours after the infusion. Blood taken from a vein and run in a laboratory using the hexokinase serum glucose method is not affected! The electrochemical strip cannot distinguish between ascorbic acid and glucose at high levels. Oral vitamin C does not have this effect. Please alert any diabetic patients of this potential complication! Diabetics wishing to know their blood sugar must have blood drawn from a vein and run in the laboratory using the hexokinase glucose determination method.
- Tumor necrosis or tumor lysis syndrome has been reported in one patient after high-dose IVC (Campbell & Jack, 1979). For this reason, the protocol always begins with a small 15 gram dose.
- Acute oxalate nephropathy (kidney stones) was reported in one patient with renal insufficiency who received a 60 gram IVC. Adequate renal function, hydration, and urine voiding capacity must be documented prior to starting high-dose IVC therapy. In our experience, however, the incidence of calcium oxalate stones during or following IVC is negligible (Riordan, et al., 2005).
- Hemolysis has been reported in patients with G6PD deficiency when given high-dose IVC (Campbell, et al., 1975). The G6PD level should be assessed before beginning IVC. (At the Riordan Clinic, G6PD readings have yielded five cases of abnormally low levels. Subsequent IVC at 25 grams or less showed no hemolysis or adverse effects.)
- IV site irritation may occur at the infusion site when given in a vein and not a port. This can be caused by an infusion rate exceeding 1.0 gram/minute. The protocol suggests adding magnesium to reduce the incidence of vein irritation and spasm.
- Due to the chelating effect of IVC, some patients may complain of shakiness due to low calcium or magnesium. An additional 1.0 mL of MgCl added to the IVC solution will usually resolve this. If severe, it can be treated with an IV push of 10 mL’s of calcium gluconate, 1.0 mL per minute.
- Eating before the IVC infusion is recommended to help reduce blood sugar fluctuations.
- Given the amount of fluid used as a vehicle for the IVC, any condition that could be adversely affected by fluid or sodium overload (the IV ascorbate is buffered with sodium hydroxide and bicarbonate) is a relative contraindication; i.e. congestive heart failure, ascites, edema, etc.
- There have been some reports of iron overload with vitamin C therapy. We have treated one patient with hemochromatosis with high-dose IVC with no adverse effects or significant changes in the iron status.
- As with any I.V. infusion, infiltration at the site is possible. This is usually not a problem with ports. Our nursing staff has found that using #23 Butterfly needles with a shallow insertion is very reliable with rare infiltrations (depending upon the status of the patient’s veins!)
- IVC should only be given by slow intravenous drip at a rate of 0.5 grams per minute. (Rates up to 1.0 gram/minute are generally tolerable, but close observation is warranted. Patients can develop nausea, shakes, and chills.)
- It should never be given as an IV push, as the osmolality at high doses may cause sclerosing of peripheral veins, nor should it be given intramuscularly or subcutaneously. The accompanying table lists the calculated osmolality of various amounts of fluid volume. Our experience has found that an osmolality of less than 1200 mOsm/kg H2O is tolerated by most patients. A low infusion rate (0.5 grams IVC per minute) also reduces the tonicity, although up to 1.0 grams per minute can be used in order to achieve higher post IVC saturation levels. (Pre and post serum osmolality measurements are advisable at this dose.)
- We presently use a sodium ascorbate solution, MEGA-C-PLUS®, 500 mg/mL, pH range 5.5-7.0 from Merit Pharmaceuticals, Los Angeles, CA, 90065.
Table 1: Recommended Dilution and Osmolarity
Table 2: Treatment Volume of Ascorbic Acid
Administration of IVC
Having taken all precautions listed above and having obtained informed consent from the patient, the administering physician begins with a series of three consecutive IVC infusions at the 15, 25, and 50 gram dosages followed by post IVC plasma vitamin C levels in order to determine the oxidative burden for that patient so that subsequent IVCs can be optimally dosed.
The initial three infusions are monitored with post IVC infusion plasma vitamin C levels. As noted above (Scientific Rational), research and experience has shown that a therapeutic goal of reaching a peak-plasma concentration of ~20 mM (350- 400 mg/dL) is most efficacious. (No increased toxicity for post IVC plasma vitamin C levels up to 780 mg/dL has been observed.) The first post IVC plasma level following the 15 gram IVC has been shown to be clinically instructive: levels below 100 mg/dL correlate with higher levels of existent oxidative stress, presumably from higher tumor burden, chemo/radiation damage, hidden infection, or other oxidative insult, such as smoking.
Following the first three IVCs, the patient can be scheduled to continue either a 25 or 50 gram IVC dose (doctor’s discretion) twice a week until the post IVC plasma level results are available from the lab. If the initial 50 gram post IVC level did not reach the therapeutic range of 350 – 400 mg/dL, another post IVC vitamin C level should be obtained after the next scheduled 50 gram IVC. If the therapeutic range is achieved, the patient is continued on a 50 gram twice a week IVC schedule with monthly post IVC determinations to assure continued efficacy. If the therapeutic range is still not achieved, the IVC dosage is increased to 75 grams of vitamin C per infusion for four infusions, at which time a subsequent post IVC plasma level is obtained. If the patient remains in a sub-therapeutic range, the IVC dosage is increased to the 100 gram level.
If after four infusions the post IVC dosage remains sub-therapeutic, the patient may have an occult infection, may be secretly smoking, or may have tumor progression. While these possibilities are being addressed, the clinician can elect to increase the 100 gram IVC frequency to three times per week. Higher infusion doses beyond 100 grams are not recommended without serum osmolality testing before and after infusions in order to properly adjust the infusion rate to maintain a near physiologic osmolality range.
If higher dosages are not tolerated, or there is tumor progression in spite of achieving the therapeutic range, lower dosages can still augment the biological benefits of IVC, including enhanced immune response, reduction in pain, increased appetite, and a greater sense of well-being.
Very small patients, such as children, and very large obese patients need special dosing. Small patients < 110 lbs. with small tumor burdens and without infection may only require 25 gram vitamin C infusions 2x/week to maintain therapeutic range. Large patients > 220 lbs. or patients with large tumor burdens or infection are more likely to require 100 grams IVC infusions 3x/week. Post IVC plasma levels serve as an excellent clinical guide to this special dosing.
In our experience, the majority of cancer patients require 50 gram IVC infusions 2-3x/week to maintain therapeutic IVC plasma levels. All patients reaching therapeutic range should still be monitored monthly with post IVC plasma levels to ensure that these levels are maintained long term. We advise patients to orally supplement with at least 4 grams of vitamin C daily, especially on the days when no infusions are given, to help prevent a possible vitamin C “rebound effect.” Oral alpha lipoic acid is also recommended on a case by case basis.
CONCLUSIONS
Vitamin C can be safely administered by intravenous infusion at maximum doses of one-hundred grams or less, provided the precautions outlined in this report are taken. At these doses, peak plasma ascorbate concentrations can exceed 20 mM.
There are several potential benefits to giving IVC to cancer patients that make it an ideal adjunctive care choice:
- Cancer patients are often depleted of vitamin C, and IVC provides an efficient means of restoring tissue stores.
- IVC has been shown to improve quality of life in cancer patients by a variety of metrics.
- IVC reduces inflammation (as measured by c-reactive protein levels) and reduces the production of pro-inflammatory cytokines.
- At high concentrations, ascorbate is preferentially toxic to tumor cells and is an angiogenesis inhibitor.
EDIT: The attached document is pretty much the same as the above post. Sorry! 
The Riordan Clinic provides a PDF document with the description of the protocol. I can't copy and paste from PDF without it looking ugly and hard to read I'm afraid.
It's 21 pages long, please see the attachment.
The Riordan Clinic provides a PDF document with the description of the protocol. I can't copy and paste from PDF without it looking ugly and hard to read I'm afraid.
It's 21 pages long, please see the attachment.
Attachments
Trending content
-

-
Thread 'Coronavirus Pandemic: Apocalypse Now! Or exaggerated scare story?'
- wanderingthomas
Replies: 30K -

-