H-kqge said:
I had been pondering whether schizophrenia was really a part of the autistic spectrum of disorders or vice versa when I first looked into autism in a serious way, but recently I haven't been able to acquire the info that could have shed a light on that idea one way or the other.
I looked into this a bit, because I was curious about cognitive slippage and autistic spectrum conditions; I've had plenty of what I think is cognitive slippage associated with vague "intuition", and have an Asperger diagnosis. The "intuition" appears in decision-making and in considering the attributes of things. I will address this issue in the second part of this post. First, the information I have found:
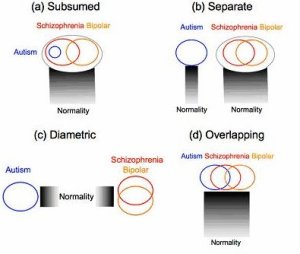
In this paper (freely accessible), a comparison is made between genetic factors associated with autism and with schizophrenia. They mention four hypotheses - (a) autism is a subset of schizophrenia; (b) they are genetically separate; (c) they are diametric opposites; (d) they partially overlap.
These hypotheses are narrowed down to two, that they partially overlap or, what they conclude is the most likely, that they are diametrically opposed: (My bolding.)
Crespi said:
We used data from studies of copy-number variants (CNVs), single-gene associations, growth-signaling pathways, and intermediate phenotypes associated with brain growth to evaluate four alternative hypotheses for the genomic and developmental relationships between autism and schizophrenia: (i) autism subsumed in schizophrenia, (ii) independence, (iii) diametric, and (iv) partial overlap. Data from CNVs provides statistical support for the hypothesis that autism and schizophrenia are associated with reciprocal variants, such that at four loci, deletions predispose to one disorder, whereas duplications predispose to the other. Data from single-gene studies are inconsistent with a hypothesis based on independence, in that autism and schizophrenia share associated genes more often than expected by chance. However, differentiation between the partial overlap and diametric hypotheses using these data is precluded by limited overlap in the specific genetic markers analyzed in both autism and schizophrenia. Evidence from the effects of risk variants on growth-signaling pathways shows that autism-spectrum conditions tend to be associated with upregulation of pathways due to loss of function mutations in negative regulators, whereas schizophrenia is associated with reduced pathway activation. Finally, data from studies of head and brain size phenotypes indicate that autism is commonly associated with developmentally-enhanced brain growth, whereas schizophrenia is characterized, on average, by reduced brain growth. These convergent lines of evidence appear most compatible with the hypothesis that autism and schizophrenia represent diametric conditions with regard to their genomic underpinnings, neurodevelopmental bases, and phenotypic manifestations as reflecting under-development versus dysregulated over-development of the human social brain.
They seem to be opposed in terms of brain development and structure, and among genes examined, four also contrast. (Duplication in two is associated with autism, whereas deletion is associated with schizophrenia; and two present the other way around.) But there are also 20 genes that overlap. In addition, whereas 2 genes have positive association with autism but not schizophrenia, 11 have positive association with schizophrenia but not autism.
When it comes to schizotaxia, I guess it's an open question whether the gene or genes responsible for that are among the ones which are opposite, the ones which otherwise differ, or the ones which overlap. And if it would be shared, what effects the differing genes have on compensation/decompensation.
Drawing upon a wider range of searching and reading, there is great individual variation in cognitive strengths and weaknesses in people on the autistic spectrum. The same also goes for idiosyncracies of thought, from obsessive-compulsive traits, to the degree of preoccupation with imagination, to disordered thought including cognitive slippage. There are also some cases of delusion, be they persecutory, grandiose, incolving hallucinations, etc.
It's been proposed that, at least in persecutory delusions, different mechanisms are at play in comparison to schizophrenics: Lack of social understanding combined with having had experiences of hostility, and tending to think of others in relation to the self and one's experiences, causes misattribution of motives and leads to forming a faulty belief system.
More generally, in part it's an open question what causes such problems in some on the autistic spectrum. Even where delusions are present, core characteristics unique to the autistic spectrum remain, both without and following successful treatment for delusions. Genetic factors might be at play; perhaps a person having the genes for the autistic spectrum, along with some selection of the otherwise non-overlapping genes for the schizo-spectrum, makes for manifesting additional schizo-features. And/or, other things may be involved. In any case, some kinds of cognitive slippage, and even more generally, highly idiosyncratic thinking, seem very common, while clinical issues of delusion are very rare.
Now I come to some speculation: To varying extents, people on the autistic spectrum can, as measured by tests, tend to underincorporate stimuli in their cognitive processing. Detail-oriented cognitive processing can also be unusually strong, while missing the "bigger picture" and having poorer comprehension. Then there are the various sensory processing issues - hypersensitivity (sometimes mixed in peculiar ways with hyposensitivity) - and, seemingly, some degree of lack of integration of sensory inputs. Could this relate to the opposite of what the schizotaxic nervous system does - instead of discrimination being inadequate, could it be excessive?
It is known (cited in the gene study at the beginning) that connectivity between different brain areas tends to be poorer than in the average brain in those on the autistic spectrum - more gray tissue, less white; greater tendency towards local processing at the cost of global. There is also, due to genetic factors, an "imbalance towards excitatory glutamatergic cortical neurotransmission." Together with excessive discrimination, if that is the case, could scattered, locally limited information together with ramped-up local processing cause cognitive errors, including some kinds of cognitive slippage, albeit on a wholly different basis?
I'll finish this part by noting my personal - introspective - experience: I've experienced that, on the one hand, I seem to have a sharp, outer "edge" to the intellect - an ability to focus on, follow and process details accurately whether or not I actually understand anything. And, on the other hand, a particularly fuzzy and sweeping intuition. (The result of information linked across the brain being somewhat limited, "coarse-grained", details not being as integrated?) But I seem to lack in what is in-between these two extremes - the processing which I think is generally the basis of insight.
This lack has become clearer over time. Only some years ago, I think it was big enough that there was no possibility of seeing it. In 2010, I had begun to "feel" it, but without understanding it - why it felt like I had no "grasp" on things, including life and all the bigger things to be understood therein in order to have a direction. That has gradually changed - at first such that I developed a poor grasp rather than having none, rather than simply following the current of life - then, now hopefully such that I have a somewhat better grasp and, in setting a direction, do not merely spin around without a clue. On a smaller scale, other changes have also been noticed in this latest stage of change, such as becoming able to understand some things I couldn't before - e.g. some mathematics, where previously all I had were the vaguest ideas and the formulas. And - becoming more self-critical.
Now for the second part, and addressing the cognitive slippage I think I've seen in myself - the problem of the vague "intuition" mentioned at the very beginning. ('The "intuition" appears in decision-making and in considering the attributes of things.' The distinction between the fuzzy intuition mentioned last in the previous section and this, is that this is a particular kind of it which interferes with thought and decision-making.)
In The Swamp, there is
an old thread of mine dealing with sensations of "energy" and the judging of the same, which is very much related. It is only a matter of whether there is an explicit labeling of what it is (a private explanation, as I then had in "energy"), or if the "intuition" persists regardless, as it has done even when questioning such old beliefs. (Only, in questioning, it has somewhat lessened in frequency and intensity.)
Basically, what it does is make some things (ideas, plans, possible actions) feel "right" and some feel "wrong". When submerged in such "intuition", there is a lack of critical-mindedness. There is often mild positive or negative feeling connected to these inner sensations, which is what makes them motivating - either pulling me towards, or away from, something. Occasionally, such feeling may be stronger. It may also be absent.
In
this recent post, I wrote about an ongoing struggle with all too often not really thinking and instead being pulled around by System 1 impulses. It quotes an earlier post, which makes reference to mental sensations. Together, these posts describe the present state of the struggle with "intuition" and uncritically being influenced by it.
I should add that in the confused thinking that can arise when submerged in this "intuition", all five of Meehl's criteria for cognitive slippage that obyvatel quoted can be fulfilled:
obyvatel said:
1) Content of construction or hypotheses intrinsically improbable.
2) Systematic failure to consider alternative hypothesis of higher antecedent probability which would explain the same allegedly “corroborating” facts.
3) Confusion between “observation” and “immediate inference” in the verbal description of an allegedly corroborating fact (e.g., patient persistently fails to consider that his perceptions of other people’s thoughts, motives or affects are, strictly speaking, not observations but inferences).
4) Handling of discorroborative data by subsuming them under multiple alternative and ad hoc hypotheses, instead of re-examining the main one.
5) At the time, definite belief, as contrasted with admittedly unreasonable, obsessional concern or preoccupation.
In this case, the automatic "conclusions" of the "intuition" are very often confused for observations. Also, for a very long time the validity of such "intuition" was an unquestioned belief; instances that could be interpreted as supporting it were used to do so, while instances that suggested it might be bunk were explained away by putting them in new, ad-hoc hypotheses. In the moment, while submerged in such "thinking", they were also the only thing considered, and as such believed in.
Being submerged in such "intuition" can further involve conflicting impulses, and as System 2 is meanwhile effectively disabled, the result is then a blank, indecisive mind, vacillating between different "intuitions". Given the sheer regularity of these instances in the past, the only difference from the following description is that the "intuitions" (while in themselves generally vague and unclear) are generally connected to something concrete, which they "represent":
obyvatel said:
Another example of cognitive slippage [...] getting perplexed and confused and mixed up in his thinking with such a high frequency that it represents a major feature of their personality. This type of confusion does not refer to being conflicted between different options which can be clearly articulated. Cognitive slippage applies when the thoughts and ideas are separately vague, scrambled or unclear. Thought deprivation or the mind going blank quite often would indicate cognitive slippage.
Fortunately, there is change regarding these things. While such "intuition" still occurs regularly, "thinking" built on top of it is now regularly questioned, and when the mind stops in the midst of a conflict of such impulses, questioning it all and breaking out of it restores thought, which can then lead to decisions. The remaining attraction to this "intuition" - what makes it come on so easily unless I focus on ignoring it and applying rational thought - is, I think, that it is both generally mildly pleasant and effortless, which has made it an ingrained automatic habit in the time since it appeared in my late teens. It can also vary widely in the level of intensity and involvement - it can be a more subtle presence in the background of the mind, and either remain so during an activity, or intensify and steal more focus. Intensity seems, on average, to more recently have weakened, though great variation remains.