Actually Malta had no deaths until yesterday. Since yesterday one 92 year old woman and one 74 year old man.Judging from those graphs, Italy, Belgium, France, and Malta all experienced a rise in excess mortality in the past month or so (though except for Italy, not reaching peaks experienced at other times in the past 4 years). Spain's excess mortality looks to be levelling off. And England and Switzerland are still experiencing rising excess mortality - again not reaching past highs.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Coronavirus Pandemic: Apocalypse Now! Or exaggerated scare story?
- Thread starter wanderingthomas
- Start date
Mandatory Intellectomy
Jedi Master
That makes no sense unless the pandemic never stops. How is a pandemic supposed to camouflage something that's been build to stay there for good? And why is there a pandemic in places that have no 5G? How does something supposedly created electromagnetically transmit to other people?The coronavirus "pandemic" is a scheme contrived to camouflage the effects of 5G being rolled out globally.
Aside from directly contradicting what the Cs said about the elite needing to actually stop the spread of the virus, how would this even work? How would tests 'infect' people without anyone noticing? If tests infect people, why are most results negative? What is the evidence for this idea?Mass testing is designed to infect people with coronavirus to perpetuate the cover story.
Those are often the worst, because of ego and their belief that they are the experts and know so much that they don't have to do any research or listen to anyone.I'm not actively engaging people, only making a remark here and there. The responses I get border on dementia. And I'm referring to scientists and researchers of my social circle.
It certainly seems like the crucial point here, as Joe explained. However, most people will never notice this stuff on their own, and the media will definitely not tell them. So the question is whether we can be loud enough about this so that even the sleeping people notice. Or whether at least some part of the mainstream-ish media will be willing to go there. It's theoretically possible to cover this up with censorship and by distracting people as usual. It also depends on how much bullshit the governments will tell us in the upcoming weeks/months.The thought came to me during work that could the miscalculation be about the death count? When people realize that the total deaths per year has not increased substantially, just shifted around. Could it be something that simple?
In relation to that, I've been thinking that it's in a way actually good if they take measures that are too strict and straight out of 1984. The more they overshoot now, the more people will notice, and the more pissed off they will be when this is over.
Ruth
The Living Force
I guess it depends where your focus of attention is. Older people and people with weak immune systems are always most at risk of dying and depending on the overall number of these people, it will influence how many die. (because they are most at risk). If there are lots and lots of these people, then death rates will increase in accordance with this number. If there aren't lots and lots of these people, then there will be no noticeable increase over and above what is normal for them.Who are the ones dying? Older people, people with weak immune systems... It isn't so much about shutting down or censoring as much as they have a system to operate from, that they can conduct - from a position of authority - problem, reaction, solution exploits. So, we don't need to concern so much about who, as we are all human resources to exploit at our level.
Though I did notice that Whitley Streiber is quoted there, which set off some alarm bells for me...but as they say, you never throw out the baby with the bathwater! I will read and study it.
Once you read, you will notice that Whitley is not quoted directly but rather his example has been used to explain how the STS bidding process works and explained rather quite well.
Yes, Topper uses Whitley as a negative example and the article itself is a MUST read in full. The following quote is the relevant one about Whitley:Whitley is not quoted with approval. Read the article.
One need only compare the behavior of truly negative beings to appreciate the difference. In the famous account of Whitley Strieber [there is] an adequate example. […]
In Strieber’s account, we witness the astonishing effort to transmute those horrific experiences into a positive outline. Thus Strieber, with almost excruciating transparency invokes the standard “humanistic” saw to the effect that dichotomies of good-and-evil are too simplistic and medieval, truth always being some “gray” blend of opposites; in this way he shields from himself the obvious implications of his ongoing ordeal.
But more importantly, he demonstrates to perfection the procedure of how one “falls into the hands” of the Negative Beings and, by the denial mechanism of 3rd density psychology, creates the belief that “good” things, developmental things, positively proceed from such ordeals. […]
His conclusions, his distillates of what he’s learned, insist almost schizophrenically that these entities must in some way have the “good of mankind” at heart, but that through the apparent terrorism of their utterly unworldly appearance and vile behavior they function something on the order of “cosmic zen masters,” taking a stick to our stubborn skulls. […] As “proof” of the actually liberating work they’re performing, Strieber invokes the fact that owing to his jarring experiences he’s “come loose” and is able to sample in waking consciousness the phenomenon of astral travel.
Strieber’s inventory of “positive side effects” on the whole describe a definitive list of what would be characterized as distinct inroads in the Negative program of conquest and ultimate Soul-capture. Like diabolical chessmen, Strieber inadvertently shows that the “space beings” have maneuvered and bullied his thoroughly beleaguered psyche into actively choosing the hypothesis with which they’ve implicitly enveloped him. […]
In further “defending” his tormentors and interpreting their tactics as a strict but ultimately benevolent discipline, Strieber helpfully displays for us one of the common vulnerabilities on which the Negative tactics count, a kind of hook upon which the Soul is sure to be snagged: the persistent intellectual pride which refuses to be counseled when the counsel seems to touch too close to truth; for any suggestion that his entities are plain evil – that he might be being deceived – seems to cause him to clutch his experiences the more covetously, and guard his interpretation jealously from any who might have a revealing word. He proclaims over and again that no one can explain his experiences to him since they’re uniquely his, that anyone with another interpretation ipso facto has an ax to grind; and finally, his intellectual superiority makes him uniquely qualified to pioneer this field which he acknowledges sharing with other “abductees,” inferentially not so well qualified.
Good to hear if Zerohedge has changed or that some of the commenters have overcome the shock. This could also signal that there are fights and discontent going on in the hierarchical elite. Something also mentioned by the C's in the last session. As time goes on with the lock-down, the stresses and thus pressure will only increase and so will the fights. Some in the hierarchy are probably experiencing something akin to The Night of the long Knives.Not even three weeks ago, most ZH commenters were COVIDIOTS. They were all-in on doing whatever it took to defeat the virus. But now, after all the dictatorial responses happening the world over, and the destruction of the FED: greater than *80%* are voicing their opinions that the whole thing is BS!! And these people are ANGRY!!
Zerohedge is surely also owned and directed by one faction of the elite and has been so from the start. Though I have never posted there, I have followed it almost daily from pretty much the beginning. As far as I know then comments are visible to non-members as I can see comments without problems.
gnosisxsophia
Jedi Council Member
Otherwise post things on social media which could perhaps make people ask questions and enjoy the show, because it truly is a giant show.
Wise words

Having neither the time, energy or inclination to engage in verbal combat, dialogue or reiteration at present. After sharing a half dozen choice selections and links gleaned from the forum, members FB posts (thanks Joe) and elsewhere, must say it was deemed strategic to retreat behind sharing the old adage;
“It is said an Eastern monarch once charged his wise men to invent him a sentence, to be ever in view, and which should be true and appropriate in all times and situations. They presented him the words:
“And this, too, shall pass away."
How much it expresses! How chastening in the hour of pride! How consoling in the depths of affliction”
And although my time and attention is, as usual, drawn far from where I would rather it be. Must say it still never fails to surprise who the individuals are that feedback constructively in contrast to those that choose otherwise...
Here a letter of a French doctor someone posted on FB. As he wants to remain anonymous, I don't know if we can give some credit, but after reading it, what he describes seems very plausible and he points out some interestings and even tragic points (see last part of the letter), especially about the people who are indirectly killed by the doctors themselves (if what he says is true, of course.)
(translated with www.DeepL.com/Translator, sorry I didn't take the time to translate it myself, but I think it's quite understandable)
"As a doctor requisitioned to help get through this epidemic crisis, I would like to share with you what is happening in the hospitals, all responding to the orders of the republic.
First of all, you should know that all public and private hospitals in the territory are empty. In this great war waged against the coronavirus, all other pathologies are relegated to second or even third place. What this means is that all scheduled hospitalizations and scheduled surgeries of people who really need care are cancelled. People who are told to stay home to avoid catching a cold end up dying at home from heart failure, for example, for which they will not have had the necessary care within a given period of time. For it should be known that this generalized panic having pushed to the confinement, with an aim of stopping the propagation of a virus "which is already there" makes that the totality of the liberal doctors, as well generalists as specialists, close their cabinet. Patients therefore no longer see a doctor, and no one can therefore assess a possible deterioration in their chronic pathology and thus refer them to a hospital service. It has therefore been more than 2 weeks in occupied France that almost all doctors and surgeons have been technically unemployed. At present, none of us understand what is happening. We all ask ourselves: "Where have these patients who fill our services all year round gone? »
Patients experiencing unusual symptoms are therefore instructed to call 15 first so that they can be told what to do: "stay home" or "go to the emergency room". Here's an example to show you the absurdity of this instruction: a patient with a slight chest pain in the right base with a slight cough and a slight fever, the 15 Centre will tell him that these are common signs of Covid-19 infection and that he should stay home, it will pass in a few days. Bad luck, it's actually a pulmonary embolism and the patient could go into hypovolemic shock at any time, in addition to necrosis of the lungs. We don't make diagnoses over the phone. Except at this time, obviously.
Now let's talk about the only hospital departments that continue to operate at full capacity: the ER and the Covid units.
The E.R. is used to screen patients with the most suspected Covid infection, or patients who may have a real life-threatening emergency that needs to be managed very quickly, as usual.
It should be noted that a Covid+ patient who is considered a "frail individual" (i.e. under 70 years of age with a significant history, or over 70 years of age) will be admitted to these Covid units.
I was requisitioned a while ago to work in one of these Units. What do they look like? The completely empty hospital wards I told you about are requisitioned to store Covid+ patients. Before being transferred from the Emergency Department to these Units, these patients are labelled: either they are under 70 years old and are labelled as "resuscitatable" (if they deteriorate, we will do everything we can to try to save them), or they are over 70 years old and are labelled LATA which means Limitation and Cessation of Active Therapeutics.
I will try to explain briefly what we do for a resuscitatable patient, and what we do for a LATA patient in this kind of situation. I remind you that the clinical picture of a severe "coronavirus" infection corresponds to pneumonia, an infection of the lungs that attacks the pulmonary alveoli. The terminal phase of this type of infection generally corresponds to what is known as septic shock with a pulmonary starting point: the germ initially present in the lungs and respiratory tract passes into the bloodstream and attacks all the vital organs: heart, brain, liver, kidneys. All of this leads to a coma that makes breathing more difficult, low blood pressure because the heart can no longer function properly, increased toxicity in the body (either because of drugs or because of waste produced by our body all the time) because the liver and kidneys no longer function.
A resuscitated patient in our department: He arrives with pure oxygen to the glasses or mask to help him breathe, we adapt the oxygen flow according to his needs (estimated by the Oxygen Saturation) and in the majority of cases: we do not touch his treatment at all! We add tablet antibiotics in some cases, they are not prescribed at all in a systematic way. The medicines he takes at home, we give them to him, and we do nothing else.
These services, which are presented to us as war zones, totally overwhelmed, are in fact surveillance units where we do almost nothing. I have never had such quiet days as I have had since this crisis began. If one of these patients starts to decompensate, to go into a state of Acute Respiratory Distress with hypotension, pseudocoma, etc. the protocol tells us to intubate, to infuse this patient with 2 to 3L of saline over 3 hours to raise the blood pressure and thus irrigate the vital organs, to give intravenous antibiotics, to give intravenous norepinephrine if the saline filling has not worked as expected. All this is to stabilize vital functions to give the antibiotics time to do their job.
I've been in emergency and resuscitation departments many times, so I know that age is not always the deciding factor when we decide whether or not to resuscitate a patient. I have already seen attempts to resuscitate patients who are 80 years old, because there is a maxim that we like to repeat to give us a clear conscience: We have an obligation of means, but no results. This means that any patient who comes into our hands, we owe it to ourselves to do everything we can to save him or her, even if it turns out to be a bad start from the beginning.
Now let's talk about the LATA patients in the Covid Unit: these are often over 70 years old. Like the young people, they come to our units with Oxygen on their nose, most often with a flow rate of 2 to 3 L/min. If these old patients ever start to require a higher flow of oxygen, 6 to 7 L/min (which can be explained by the fact that these old patients have been carrying their pneumonia for about 7 days most of the time, as they are ordered to stay at home), it is considered that they will not survive their infection. 6 or 7 L/min of oxygen is the limit between life and death in these Units. Once this stage is reached, the LATA label comes into play. Considering that these old people are going to die anyway (since they will not be resuscitated, cuckoo the obligation of means), we inject them with a cocktail of Morphine and Hypnovel intravenously. We also use these two molecules in Palliative Care: they induce an artificial coma, a well-known effect, and they also have a respiratory depressive effect. In fact, they have a muscular relaxing effect, particularly on the respiratory muscles (diaphragm, intercostal muscles, pharyngeal muscles, etc.) and therefore lead to drug-induced asphyxia. Doctors, so attached to ethics, call this a "sweet death". In these units, we therefore artificially kill patients who are condemned as soon as they leave the emergency room. At no time do we seek to do medicine with them.
These deaths are then counted as victims of coronavirus, whereas they are in fact the victims of French doctors.
The families of these victims cannot even realize anything. With this confinement, the young patients are not allowed any visits. Patients at the end of life (those who have benefited from the LATA cocktail), are entitled to only one visit per day. The relatives must therefore agree on who will visit the future dead person. And this visitor will not be allowed to visit again during the current week. They therefore have no way to appreciate the clinical evolution of their relative, because we rarely hold more than a week under Morphine and Hypnovel.
So our policies are orchestrating a lot of hospital deaths, and using these deaths to create a general psychosis for a purpose that I cannot yet visualize.
Translated with www.DeepL.com/Translator (free version)
Can you provide the link in French?
This letter really nails what is going on and it is horrifying. This thing should be copied and everyone should send a copy to their doctor(s).
It should be on SOTT if it isn't already, and spread far and wide on social media.
This thread.
Only 8 pages of posts today.
The curve is flattening.")
LOL!
Yes, I'm actually getting bored by the whole thing though I know I need to keep track of new developments just to see what those evil bastards are up to next.
Ruth
The Living Force
I agree. I think it's a scheme to camouflage the effects of mandatory vaccinations being rolled out globally. It's like people are saying "Look at that storm!" and I respond "Well that's nice. How about that Cat 5 Hurricane due to hit landfall any time now? Can anyone see that?"The coronavirus "pandemic" is a scheme contrived to camouflage the effects of 5G being rolled out globally.
That makes no sense unless the pandemic never stops. How is a pandemic supposed to camouflage something that's been build to stay there for good? And why is there a pandemic in places that have no 5G? How does something supposedly created electromagnetically transmit to other people?
More priming for what's coming:
Didn't manage to edit the post in time. Here is the rest:
More priming for what's coming:

Violent extremists may exploit coronavirus pandemic, target hospitals, threat report warns - National | Globalnews.ca
ISIS and right-wing extremist propaganda have encouraged exploiting the health crisis but such attacks may be impractical.
 globalnews.ca
globalnews.ca
Violent extremists may try to take advantage of the coronavirus pandemic by attacking hospitals and supermarkets, according to a U.S. threat assessment circulated in Canada by the RCMP.
“Pandemics and other natural crises create unprecedented challenges that terrorists could exploit to conduct attacks against and already stressed society, and strained government and public safety system,” it said.
“While most citizens isolate in their homes, public safety personnel, hospitals and establishments, such as supermarkets and pharmacies, serve the largest number of co-located individuals, making them potentially attractive targets.”
I thought they are now using technology to monitor everybody's social distancing. The same technology cannot be used to track these extremists? Who are they?
On April 1, U.S. authorities said they had arrested a 44-year-old conspiracy theorist for running a locomotive off the end of its tracks near a navy hospital ship treating COVID-19 patients in the port of Los Angeles.
Ah... those guys...
The report also included an April 1 Department of Homeland Security (DHS) assessment of attempts by extremists to encourage supporters to spread COVID-19 to law enforcement members and minority communities, as well as at places of worship and on public transit.
OK, so these extremists and their supporters are either already infected, and they know it, or have means to become infected in order to support the cause.
But then further down in the same article they say:
But the report also said medical facilities may not be a “favorable environment” for violent extremists, and they lack experience with such targets. They may also fear contracting the virus themselves.
Huh??
“The lack of quantifiable success and possible violent extremist actors’ concerns for their own health may feed into the decision calculus to seek out exposure to infect others.”
It also noted that since those with COVID-19 do not always develop symptoms, violent extremists would not necessarily know they were infected, making it impossible for them to attempt to intentionally infect others.
for the sake of accuracy man was in fact 79 and riddled with all sorts of health problems.Actually Malta had no deaths until yesterday. Since yesterday one 92 year old woman and one 74 year old man.
Thinking about what Dr. Shiva said and vitamin D being essential for immune defense I could hypothesize that one of the reasons Malta is so mildly hit is because of year round exposure to sunshine.
Persephone
Jedi Master
Here is the link received by my friend in his FB:Can you provide the link in French?
This letter really nails what is going on and it is horrifying. This thing should be copied and everyone should send a copy to their doctor(s).
It should be on SOTT if it isn't already, and spread far and wide on social media.
Here is the link of the original post but it has been removed
 www.facebook.com
www.facebook.com
Ruth
The Living Force
Distraction and Camouflage? This is to stop people looking in the right direction.So why on Earth would anyone assert that "5G did it"?

Nearly half a billion people may end up in poverty due to coronavirus crisis: report - National | Globalnews.ca
Under the most serious scenario - a 20% contraction in income - the number of people living in extreme poverty would rise by 434 million people to 922 million worldwide.
globalnews.ca
The fallout from the coronavirus spread that has killed more than 83,000 people and wreaked havoc on economies around the world could push around half a billion people into poverty, Oxfam said on Thursday.
“The economic crisis that is rapidly unfolding is deeper than the 2008 global financial crisis,” the report found.
You think? You need a special report in order to figure that one out?
“The estimates show that, regardless of the scenario, global poverty could increase for the first time since 1990,” it said, adding that this could throw some countries back to poverty levels last seen some three decades ago.
To help mitigate the impact, Oxfam proposed a six point action plan that would deliver cash grants and bailouts to people and businesses in need, and also called for debt cancellation, more IMF support, and increased aid. Taxing wealth, extraordinary profits, and speculative financial products would help raise the funds needed, Oxfam added.
Calls for debt relief have increased in recent weeks as the fallout from the COVID-19 pandemic has roiled developing nations around the world.
“Rich countries have shown that at this time of crisis they can mobilize trillions of dollars to support their own economies,” the report said.
“Yet unless developing countries are also able to fight the health and economic impacts the crisis will continue and it will inflict even greater harm on all countries, rich and poor.”
So looks like a Global bailout is coming as well.
The crisis is maintained by the WHO and its sister IMF will bring the second wave soon.
Some gleanings from the past few days of things that caught my eye and I posted on my FB wall if anybody wants to go over and share.

 www.rt.com
www.rt.com

 www.rt.com
www.rt.com

 www.rt.com
www.rt.com

 wattsupwiththat.com
wattsupwiththat.com

 www.theepochtimes.com
www.theepochtimes.com

 www.thegatewaypundit.com
www.thegatewaypundit.com

 www.grassfire.com
www.grassfire.com
 wattsupwiththat.com
wattsupwiththat.com

 www.rt.com
www.rt.com
 www.zerohedge.com
www.zerohedge.com

 www.mercurynews.com
www.mercurynews.com

 www.redstate.com
www.redstate.com

 www.newsbusters.org
www.newsbusters.org

 www.thegatewaypundit.com
www.thegatewaypundit.com
 www.thegatewaypundit.com
www.thegatewaypundit.com

 www.theguardian.com
www.theguardian.com

 www.politico.eu
www.politico.eu
This one is VERY interesting:
 www.thegatewaypundit.com
www.thegatewaypundit.com

 www.breitbart.com
www.breitbart.com

 www.rt.com
www.rt.com

 wholefoodsmagazine.com
wholefoodsmagazine.com
 www.breitbart.com
www.breitbart.com

 www.forbes.com
www.forbes.com
www.zerohedge.com
Rice & wheat prices surge amid fears Covid-19 lockdown may threaten global food security
Rice & wheat prices surge amid fears Covid-19 lockdown may threaten global food security
What did they know, exactly? US intel warned of ‘cataclysmic’ coronavirus pandemic in NOVEMBER 2019, report claims
US military intelligence tried to raise the alarm about the coronavirus epidemic in China when it was still embryonic in November, inside sources claim – raising questions of what they knew and who ignored, or squashed the report.
France to extend coronavirus lockdown beyond April 15
Coronavirus lockdown measures in France, already in place for more than three weeks, will be extended further, President Emmanuel Macron’s office said. The country has filed over 110,000 confirmed cases and 10,800 deaths.
Coronavirus Death Predictions Bring New Meaning to Hysteria
image licensed from 123rf.com Reposted from RealClearMarkets with author permission (and slightly out of date) By Michael Fumento April 01, 2020 The U.S. is staring at a Netflix-type apocalypse. Y…
COVID-19 Death Toll Will Be ‘Much Lower’ Than Projected, Top Officials Say

Trump Looking Into Reopening Parts Of US Economy, Treasury Secretary Says | The Gateway Pundit | by Eric A. Blair
Treasury Secretary Steven Mnuchin said on Tuesday that President Trump is looking into reopening parts of the U.S.

This Is Strange: Total US Deaths in March 2020 are Actually Down 15% from Average of Prior Four Years
What is going on? After shutting down the government and killing the greatest economy in the world due to deathly estimates from specialists on the coronavirus, the data is showing that this may be one great big mistake or hoax. Grassfire reports: According to data obtained from the CDC’s...www.thegatewaypundit.com
Grassfire reports:
Now after deaths for the entire month of March are reported, the results show that deaths in the US this March are 15% less than the average of the past four years!According to data obtained from the CDC’s National Center for Health Statistics Mortality Surveillance System website, total U.S. deaths for the first three weeks of March are DOWN 10% from the average of the prior four years for the same three week period.
The average for weeks 9 through 11 for the four prior years was a total of 170,555 deaths. For weeks 9 through 11 this year, the total is 153,015, meaning 17,540 fewer people died in America during the first three weeks of March than could be reasonably expected. And the gap between historic deaths and weekly deaths is widening. For week 11, just 47,655 Americans died, 8,773 and 15% fewer than the average for week 11 in the prior four years. And while data on week 12 is not complete, it is trending similar to week 11 and will likely be down by 15% (around 8,700 deaths less than expected) even though 1,919 COVID-19 deaths were reported (in week beginning 3/22).
What? Total U.S. Deaths DOWN 10% In March From Prior Years, Further Raising Question Of COVID Impact
Million Strong. Standing For America.
www.grassfire.com
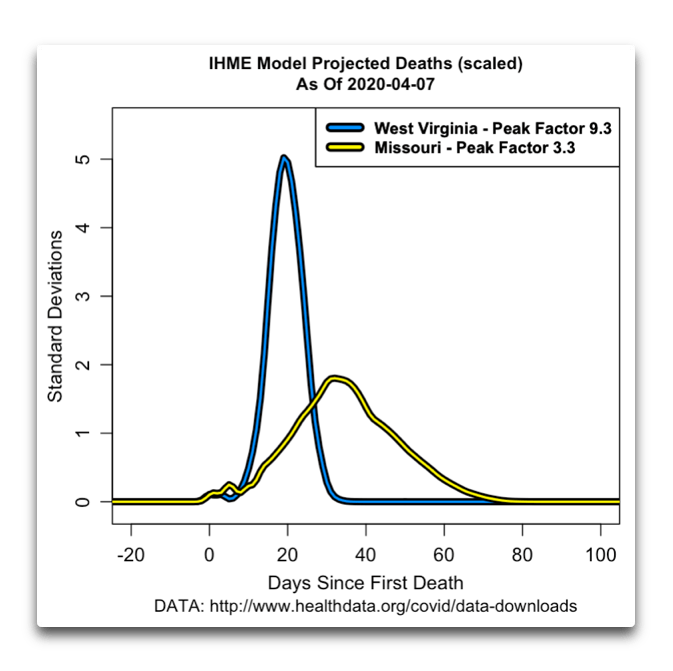
Flattening The Curve
Guest Post by Willis Eschenbach I’ve been following the many changes in the IHME coronavirus model used by our very own most incompetent Dr. Fauci. (In passing, let me note that he’s be…
Covid-19 drags French economy into deep recession the likes of which it has not seen since 1945
Covid-19 drags French economy into deep recession the likes of which it’s not seen since 1945
ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
California surfer in handcuffs after enjoying empty, epic waves
Some surfers would do anything to ride waves at perfect Malibu – an iconic spot usually packed with people – with no one else out.
www.mercurynews.com
Flashback: Let's Watch How CNN, MSNBC, and Other *Non-Fox News* Networks Downplayed the Wuhan Virus
CNN was among the worst offenders.
www.redstate.com
Harbingers of DOOM: CBS Decries Trump’s Messages of HOPE in Crisis
President Trump drew the ire of CBS Evening News and White House correspondent Weijia Jiang on Monday for daring to keep American spirits up, and letting them know there was “light at the end of the tunnel.” Citing unnamed “experts,” Jiang decried Trump’s optimism by claiming the country wasn’t...
www.newsbusters.org





"This Man is My Father" - Dr. Marc Siegel Defends the Hydroxychloroquine Treatment for Coronavirus with the Most Moving Story Imaginable (VIDEO)
Dr. Marc Siegel, FOX News Medical Correspondent joined Tucker Carlson on Tuesday night to discuss the hydroxychloroquine treatment for the coronavirus. Several studies have shown tremendous success with hydroxychloroquine and Z-Paks to treat the virus. Dr. Marc Siegel ended the segment with this...
Dr. Marc Siegel ended the segment with this moving testimonial.
Dr. Siegel: Tucker, I want to tell you about a 96-year-old man in Florida who one night, “I don’t think I’m going to make it. I feel very weak. The end is coming. I’m coughing. I’m short of breath. I can’t get up from the couch.” The next day he was on hydroxychloroquine and antibiotics per his cardiologist. He got up the next day he was fine. This man is my father.
Dem Lawmaker Who Credited Trump For Saving Her Life Says She Had to Beg For Hydroxychloroquine After Michigan Gov Barred the Drug (VIDEO) | The Gateway Pundit | by Cristina Laila
A Democrat state lawmaker from Michigan credited hydroxychloroquine and President Trump for saving her life in her battle with the Coronavirus.
Doctor Prescribing Hydroxychloroquine Says All of His "Very, Very Ill" Patients with Coronavirus Became Symptom Free within 8-12 Hours (VIDEO) | The Gateway Pundit | by Cristina Laila
A Los Angeles doctor prescribing hydroxychloroquine in conjunction with zinc is seeing a 100% success rate with every patient he has treated suffering from the Coronavirus.

Inside the epic White House blowup over "game-changer" hydroxychloroquine
The drama pitted economic adviser Peter Navarro against infectious disease expert Anthony Fauci.www.axios.com
Behind the scenes: This drama erupted into an epic Situation Room showdown. Trump's coronavirus task force gathered in the White House Situation Room on Saturday at about 1:30pm, according to four sources familiar with the conversation. Vice President Mike Pence sat at the head of the table.
Toward the end of the meeting, Hahn began a discussion of the malaria drug hydroxychloroquine, which Trump believes could be a "game-changer" against the coronavirus.
- Numerous government officials were at the table, including Fauci, coronavirus response coordinator Deborah Birx, Jared Kushner, acting Homeland Security Secretary Chad Wolf, and Commissioner of Food and Drugs Stephen Hahn.
- Behind them sat staff, including Peter Navarro, tapped by Trump to compel private companies to meet the government's coronavirus needs under the Defense Production Act.
Navarro's comments set off a heated exchange about how the Trump administration and the president ought to talk about the malaria drug, which Fauci and other public health officials stress is unproven to combat COVID-19.
- Hahn gave an update about the drug and what he was seeing in different trials and real-world results.
- Then Navarro got up. He brought over a stack of folders and dropped them on the table. People started passing them around.
- "And the first words out of his mouth are that the studies that he's seen, I believe they're mostly overseas, show 'clear therapeutic efficacy,'" said a source familiar with the conversation. "Those are the exact words out of his mouth."
Fauci's mention of anecdotal evidence "just set Peter off," said one of the sources. Navarro pointed to the pile of folders on the desk, which included printouts of studies on hydroxychloroquine from around the world.
- Fauci pushed back against Navarro, saying that there was only anecdotal evidence that hydroxychloroquine works against the coronavirus.
- Researchers have said studies out of France and China are inadequate because they did not include control groups.
- Fauci and others have said much more data is needed to prove that hydroxychloroquine is effective against the coronavirus.
- As part of his role, Navarro has been trying to source hydroxychloroquine from around the world. He's also been trying to ensure that there are enough domestic production capabilities inside the U.S.
Navarro started raising his voice, and at one point accused Fauci of objecting to Trump's travel restrictions, saying, "You were the one who early on objected to the travel restrictions with China," saying that travel restrictions don't work. (Navarro was one of the earliest to push the China travel ban.)
- Navarro said to Fauci, "That's science, not anecdote," said another of the sources.
Between the lines: "There has never been a confrontation in the task force meetings like the one yesterday," said a source familiar with the argument. "People speak up and there's robust debate, but there's never been a confrontation. Yesterday was the first confrontation."
- Fauci looked confused, according to a source in the room. After Trump imposed the travel restrictions, Fauci has publicly praised the president's restriction on travel from China.
- Pence was trying to moderate the heated discussion. "It was pretty clear that everyone was just trying to get Peter to sit down and stop being so confrontational," said one of the sources.
- Eventually, Kushner turned to Navarro and said, "Peter, take yes for an answer," because most everyone agreed, by that time, it was important to surge the supply of the drug to hot zones.
- The principals agreed that the administration's public stance should be that the decision to use the drug is between doctors and patients.
- Trump ended up announcing at his press conference that he had 29 million doses of hydroxychloroquine in the Strategic National Stockpile.
The bottom line: The way to discuss the drug's potential has become a fraught issue within the Trump administration.
- In response to a request for comment on Axios' reporting, Katie Miller, a spokesperson for the vice president, said: "We don't comment on meetings in the Situation Room."
- Most members of the task force support a cautious approach to discussing the drug until it's proven.
- Navarro, on the other hand, is convinced based on his reading that the drug works against the coronavirus and speaks about it enthusiastically.
- Some of Trump's favorite TV hosts, including Fox's Sean Hannity, and friends including Rudy Giuliani, have also been touting the malaria drug for the coronavirus. Trump has made no secret who he sides with.
- "What do you have to lose? Take it," the president said in a White House briefing on Saturday. "I really think they should take it. But it's their choice. And it's their doctor's choice or the doctors in the hospital. But hydroxychloroquine. Try it, if you'd like."
Controversial drug hydroxychloroquine to be given to coronavirus patients in Australia
Infectious diseases experts urge caution amid concerns about anti-malarial’s possible side-effects
EU science chief resigns, slamming bloc’s coronavirus response
Mauro Ferrari cites ‘internal political thunderstorm’ in response to his proposals.
www.politico.eu
This one is VERY interesting:

A report by Italian physicians found similarly serious cardiac issues associated with the coronavirus outbreak. An “otherwise healthy 53-year-old patient” developed myocarditis, a serious inflammation in the heart, just a week after experiencing fever and a dry cough due to COVID-19. [...]
“We were thinking lungs, lungs, lungs — with us in a supportive role,” John Rumsfeld, chief science and quality officer at the American College of Cardiology, told the Times. “Then all of a sudden we began to hear about potential direct impact on the heart.” [...]
“We have to assume, maybe, that the virus affects the heart directly,” Jorde told SA. “But it’s essential to find out.”

CBS News Posts Fraudulent Viral Video of Sobbing ICU Nurse Who Quit Her Job Over Poor Working Conditions, Mask Shortage -- It Was All a Lie | The Gateway Pundit | by Cristina Laila
CBS News was caught once again posting a fraudulent video to make it look like President Trump is failing in his response to the Coronavirus pandemic.
Study: Smokers Appear Less Likely to Be Hospitalised with COVID-19
Smoking may reduce the likelihood of being hospitalised with coronavirus, claim researchers at the University of West Attica and NYU.
www.breitbart.com
Trump vows to put ‘very powerful hold’ on US funding to WHO over response to Covid-19
US President Donald Trump has threatened to hold back funding to the World Health Organization, potentially leaving the agency without support from its largest donor as many of its 194 members are being ravaged by the coronavirus.
Nevada Gov Orders Closures of Health Food Stores; NPA Responds - WholeFoods Magazine
UPDATE April 8, 2020: As of 7:45 AM EST, the order to close health food stores has not been lifted for the state of Nevada, according to the NPA. The association told WholeFoods Magazine in an email that Nevada Governor Steve Sisolak and Nevada Attorney General Aaron Ford have not changed their...
Epidemiologist Dr. Knut Wittkowski: ‘Without Lockdowns the Covid-19 Epidemic Would Have Been Over by Now’
What an interview! Wittkowski doesn't mince words or sugarcoats anything. This is an almost ruthlessly direct man. He says not doing anything in particular about Covid-19 would have killed 2% of all cases with symptoms, but lockdowns are going to drawww.anti-empire.com
He also has the first plausible explanation of what happened in Wuhan and why the Chinese were able to finally seemingly contain it (the outbreak had burned itself out, as leaving schools open very late into the outbreak laid the groundwork for herd immunity to build). Worth a watch:
Delingpole: Trump Offers Boris Coronavirus Drugs Not Available on NHS
I wish I could say Boris Johnson was getting the best available treatment. But given that the NHS is involved, I somehow doubt it.
www.breitbart.com
Coronavirus Is The ‘Largest Insolvency Event’ In History, Warns Former Goldman Sachs Fund Manager—Pivots Hard To Bitcoin
Renowned former Goldman Sachs fund manager Raoul Pal has warned the coronavirus crisis will cause "the largest insolvency event in all history," while moving 25% of his portfolio to bitcoin...
www.forbes.com
ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
Sorry if this has been posted already however I haven't seen it posted on this thread.
Continuing with the theme of unmasking Bill Gates, Robert F. Kennedy junior yesterday posted this instagram post which I have copied below.
I know Dr. Shiva is not a huge fan of Robert Kennedy Junior and appears to believe that he may be a gatekeeper in regards to vaccines or some sort of controlled opposition due to his previous support of HIllary Clinton and her known involvement with promoting vaccines, although this may be due to his loyalty to the democrat party, or perhaps he has since changed his tune I am not sure . His instagram post does detail many harmful aspects of Bill Gate's vaccine programs, which are quite revealing, so FWIW.
I have only copied the first page of his post on Bill Gates, the other 2 pages are on his second and third instagram images.
Continuing with the theme of unmasking Bill Gates, Robert F. Kennedy junior yesterday posted this instagram post which I have copied below.
I know Dr. Shiva is not a huge fan of Robert Kennedy Junior and appears to believe that he may be a gatekeeper in regards to vaccines or some sort of controlled opposition due to his previous support of HIllary Clinton and her known involvement with promoting vaccines, although this may be due to his loyalty to the democrat party, or perhaps he has since changed his tune I am not sure . His instagram post does detail many harmful aspects of Bill Gate's vaccine programs, which are quite revealing, so FWIW.
I have only copied the first page of his post on Bill Gates, the other 2 pages are on his second and third instagram images.
Trending content
-

-
Thread 'Coronavirus Pandemic: Apocalypse Now! Or exaggerated scare story?'
- wanderingthomas
Replies: 30K -
-
